COLDS
Comprehensive guide on epidemiology, microbiology, pathogenesis, symptoms, diagnosis, and treatment of common colds and the flu. Learn about misconceptions and antibiotic resistance.

COLDS
E N D
Presentation Transcript
COLDS Matt Love
TheCOMMONCold • #1 REASON for visits to physicians, #3 for internists • 27 million physician visits per year • 23 million days of work missed • Average adult has 2-4 colds per year • $3 billion spent per year on OTC remedies
Epidemiology • September through May • Spread by hand-to-hand contact and aerosols
Microbiology Virus % of cases Rhinovirus 30-40 Coronavirus 10-15 RSV Influenza Parainfluenza Adenovirus Unkown 25-40
Pathogenesis • ICAM • Rhinosinusitis • Histology of Nasal Epithelium is Normal • Increased vascular permeability and secretions • Components of Snot • Role of PMNs, Histamine, Kinins, IL
Approach to the common cold • H & P • Diagnosis - consider complications, flu allergy, strep • Ascertain Expectations • Reassure (but don’t minimize) • Express sympathy • Educate • Offer symptomatic relief
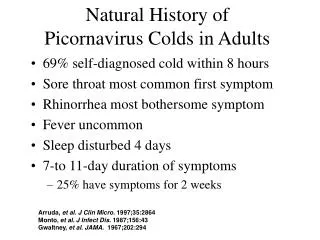
H & P SymptomFrequencyDay Nasal 45 to 75% 1 - 2 Discharge Sneezing Obstruction Pharyngeal 35 to 50% 2 - 3 Sore Throat Scratch Throat Cough 40 to 80% 2 -14 Hoarse 15 to 30% 2 - 14 Constitutional 2 - 4 Feverish Myalgia Headache
Consider Complications • Bronchitis • Sinusitis • Otitis Media • Pneumonia • Bronchospasm
THE TRUE BLUE FLUEpidemiology • Usually peaks in January or later • 20,000 deaths in a typical epidemic season • 110,000 hospitalizations • 10%-20% of population infected during typical season • When flu epidemic in region, high percentage of those with ILI have flu
THE TRUE BLUE FLUClinical Presentation • Classic Flu - sudden onset prostration, high fever, nasal stuffiness, sore throat, myalgia, cough and headache • Study Flu - usually fever + 2 symptoms • Illness resolves over four to five days • Cough, fatigue, malaise can linger 2-3 weeks • Complications - bacterial tracheobronchitis, sinsusitis, pneumonia
Symptom Fever (> 37.8) Feverishness Cough Nasal congestion Weakness Loss of Appetite Sore Throat Headache Myalgia With fluWithout flu 68 40 90 89 93 80 91 81 94 94 92 86 84 84 91 89 94 94 DIAGNOSIS OF INFLUENZAAre there pathognomonic symptoms?Proportion of patients with symptom
DIAGNOSIS OF INFLUENZAAre there pathognomonic symptoms? USE OF A CASE DEFINITION AS A DIAGNOSTIC TOOL 100 patients with a flu-like illness: T > 37.8 plus 2 of 4: cough, myalgia, sore throat, headache Case Definition: T > 38 + cough during flu season Positive Predictive Value 86.8% Negative Predictive Value 39.3% Sensitivity 77.6% Specificity 55.0% __________________________
DIAGNOSIS OF INFLUENZA INFLUENZA SURVEILLANCE\ www.cdc.gov • WHO - worldwide tracking of drift and shift • CDC, Influenza Branch • National Respiratory and Enteric Virus Surveillance System • 122 Cities Mortality Reporting System • State and Territorial Epidemiologists Reports • US Influenza Sentinel Physicians Surveillance Network
DIAGNOSIS OF INFLUENZA RAPID FLU TESTS
INFLUENZA Treatment Drug Trade Name Flu Type Cost Caveat ____________________________________________________ Amantidine Symmetrel A 9.83 Resistance Generic 1.72 CNS Rimantidine Flumadine A 18.87 Resistance Zanamivir Relenza A and B 44.40 Bronchospasm Oseltamivir Tamiflu A and B 53.00 GI
INFLUENZA Prophylaxis • VACCINATE • EXPOSURES • LONGTERM CARE FACILITIES
Approach to the common cold • H & P • Diagnosis - consider flu, bacterial complications, allergy, strep • Ascertain Expectations • Reassure (but don’t minimize) • Express sympathy • Educate • Offer symptomatic relief
Patients’ Understanding of the Common Cold * 87% of people do not seek care for their colds * In a survey of young adults 94% said it was not necessary to go to a doctor for a cold. On the other hand * Of patients in a clinic for other reasons, 61% said they would seek care for 5days rhinorrhea, cough, sore throat; if the discharge were discolored, 79% would seek care. * 87% of a sample in England thought antibiotics were beneficial for a cold. a
Patients’ Understanding of the Common Cold What Causes a Cold? Virus 43.5% Virus and Bacteria 41.9% Bacteria 7.9% Don’t Know 6.7% Antibiotics are helpful for colds Strongly Agree 18.2% Agree 26.1% Disagree 17.2% Strongly Disagree 31.4% Don’t know 7.1% aa
Factors Correlating with a Desire for Antibiotics • Previous Rx for Antibiotic for URI • Belief they work • Purulent secretions • Medicaid • From a country where abx are OTC
Why not give antibiotics? Biggest Risk Factor for developing resistant S.pneumonia is previous exposure to abx Good studies show that when overall antibiotic prescribing is reduced, the prevalence of resistant strains drops. About 30% of all the antibiotics prescribed in the US are for outpatient colds. In many studies, patients with clear cut colds are Rxed abx 50-60% of the time. They don’t work a
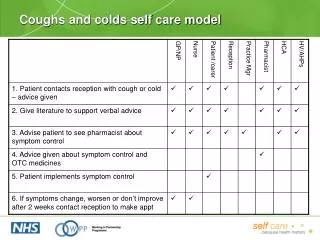
A Multidimensional Intervention to Reducing Rxs For Antibiotics • For “Bronchitis” • Preliminary study found that clinicians code according to Rx given, not symptoms. The dx of “chest cold” rather than “bronchitis” lowered expectations for abx • Patient and clinician education • Reduced Rxs for bronchitis from 74% to 48%
Symptomatic Treatment SymptomTreatments Congestion Topical Decongestant Oral Decongestant Rhinorrhea Anticholinergic Sneezing Antihistamine Cough Suppressant Tx for Rhinorrhea Constitutional Acetaminophen ASA, NSAID Sore Throat Gargles, Lozenges Analgesia a
Remedies • Zinc Gluconate • Vitamin C • Chicken Soup • Vapors
Your body’s immune system works bestwhen yougive it plenty of rest
In the meantime, let’s see if we can treat the symptoms so you’re not suffering so much.
Approach to the common cold • H & P • Diagnosis - consider complications, flu allergy, strep • Ascertain Expectations • Reassure (but don’t minimize) • Express sympathy • Educate • Offer symptomatic relief