Download
1 / 56
680 likes | 1.24k Vues
Pharmacology of Hormones Endocrine Pancreas. Martin Sterba, PharmD.,PhD. Dept. of Pharmacology. Glucagon. Polypeptide hormone (29AA) Secreted by pancreatic α -cells Secretion is stimulated by : low plasma glucose , high plasma AA …

E N D
Pharmacology of HormonesEndocrine Pancreas Martin Sterba, PharmD.,PhD. Dept. of Pharmacology
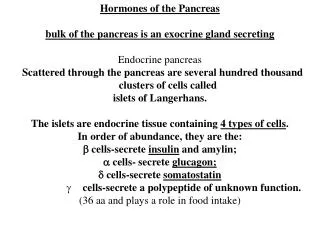
Glucagon • Polypeptide hormone (29AA) • Secreted by pancreatic α-cells • Secretion is • stimulated by: low plasma glucose, high plasma AA… • secretion is inhibited by: high plasma glucose, insulin, somatostatin… • Mechanism of Action: binds on Glucagon receptors (GPCR type) on hepatocytes → increased cAMP →PK A →→ glycogen phosphorylase →release of glucose from glycogen • Metabolic effects: catabolic hormone - increased glycogenolysis and gluconeogenesis result in increased plasma glucose levels
Pharmacological use of glucagon • All parenteral routes of administration are feasible • i.v., i.m., s.c. • Main indication:vital first aid in hypoglycemia • When patient is unconsciousness (cannot take glucose syrup orally) • When i.m./s.c. route of drug administration is needed e.g., acute first aid provided by non-medical personnel or i.v. route is not available • The response is relatively rapid (within 2 min after i.v.glycemia increases promptly), duration of action: 10-20 min.
Pharmacological use of glucagon • Other indications: • treatment of b-blocker-induced overdose associated with severe bradycardia, heart failure or hypotension • indirect antagonisms of decreased cAMP leads to restoration of contractility a normal HR • High doses needed! • Compare half-lives for b-blockers (2-12h) and glucagon (5-15min) • used empirically in emergency setting to overcome severe myocardial depression non-responding to standard treatment • Adverse effects • generally acceptable • headache, nausea, hyperglycemia
Insulin and pharmacology of diabetes mellitus • Insulin biochemistry • polypeptide hormone (51AA) • Synthesized and released by β-cells representing 60-80% of Islet of Langerhans cells • Biosynthesis in following steps: 1. preprosinsulin 2. proinsulin 3. insulin • C-peptide plasma marker of insulin secretion
Factors regulating insulin secretion INTESTINE Digested food BLOOD Glucose Amino acids Fatty acids Sulfonylureas GIT hormones Parasympathetic nerves (on muscarinic receptors) D cell Somatostatin B cell Glucagon A cell Sympathetic nerves and adrenaline (on a2-adrenoceptors) PANCREATIC ISLET Amylin Insulin
The effect of hormones on blood glucose Main stimulus for secretion Main effect Main actions Hormone Main regulatory hormone Insulin Glucose uptake Glycogen synthesis Acute rise in Blood Glycogenolysis blood glucose glucose Gluconeogenesis Main counter-regulatory hormones Glucagon Glycogenolysis Gluconeogenesis Adrenaline Glycogenolysis Glucose uptake Glucocorticoids Glyconeogenesis Glucose uptake and utilisation Growth hormone Glucose uptake Hypoglycaemia (i.e. blood glucose < 3 mmol/l) e.g. with exercise, stress, high protein meals, etc. Blood glucose
Insulin receptors • Insulin receptors are cell surface receptors with protein kinase activity • They are responsible for both physiological and pharmacological action of insulin and its analogues
Diabetes mellitus - Diabetes is not a single disease • It is rather a heterogeneous group of syndromes characterized by an elevation of blood glucose andmetabolic perturbation caused by a relative or absolute insulin deficiency • Main types: • Type I – insulin-dependent DM • Type II – non-insulin-dependent DM • Other types • Maturity-onset DM of the young (MODY) • Gestational diabetes…
Diabetes diagnosis and glycemia • Fasting Plasma Glucose (FPG): <5.6 mmol/l = normal glycemia 5.6 - 6.7 mmol/l = impaired glucose tolerance > 6.7 (7) mmol/l = diabetes mellitus • Glucose tolerance test (2h postprandial glucose) > 11 mmol/l diabetes mellitus
Type I DM • 5-10% of all patients diagnosed with DM • Strong genetic background • Typical onset – juvenile (around puberty), but may occur at any age • Pathogenetic mechanisms – loss of β-cells or their function due to the autoimmune mechanisms, toxic damage etc. • Endocrine pancreas fails to respond to increased glucose levels by insulin secretion – insulin levels are very low • It results into the acute or chronic hyperglycemia • Symptoms: marked polyuria, polydipsia, weight loss…
Type I DMPharmacotherapy • Appropriate substitution therapy with exogenous insulin or insulin analogues is a must (IDDM) to avoid: • acute complications • diabetic ketoacidosis (potentially life-threatening) • chronic complications • peripheral neuropathies, • microangiopathies (nephropathies, retinopathies) • macroangiopathies (accelerated atherosclerosis which leads into myocardial ischemia, cerebral ischemia, lower extremity ischemia…)
Type I DMPharmacotherapy • AIM: to maintain blood glucose as close to normal as possible, and to avoid wide swings in their levels (that contribute to long-term complications). • Deserves adherence to special diet and regular living habits • Compliance is essential! • Standard therapy – twice daily • Intensive therapy – 3 or more daily doses • Usually combination of short acting insulin (mimic post prandial insulin secretion) and long acting preparations (basal secretion, antagonizeglucose released from the liver) • Therapy monitoring: blood glucose (self-monitoring improves compliance), glycated hemoglobin(HbA1c).
Type II DM (NIDDM) • Much more frequent than Type I! • Besides genetic component, living habits, obesity and aging play an important role • Typical onset in elderly Pathogenesis • B-cells are not destroyed (at least not primarily) • Insulin secretion impairment and/or loss of tissue sensitivity to insulin (insulin resistance) are the key issues here • This leads to inability to maintain proper glucose homeostasis • The symptoms and complications are similar to DM type I, but less acute/severe and obvious • E.g. marked ketoacidosis is rare
Type II DM (NIDDM)Pharmacotherapy • AIM: To maintain blood glucose within normal limits and to prevent the development of chronic complications. • Diet + weight reduction + pharmacological approach • Important part of complex therapeutic approach to Metabolic syndrome • Drugs in Type II DM – oral hypoglycemic agents = standard treatment! – insulin (rather in specific situations only) • acute complications (stress, infection, surgery, disease, pregnancy) • when the disease is finally worsening beyond manageability with oral hypoglycemics
Release of insulin that occurs in response to the constant infusion of glucose in normal subjects and diabetic patients Normal subjects 80 Type 2 diabetes 40 Plasma concentration of insulin (mg/mL) Type 1 diabetes 0 0 5 10 Minutes Infusion of glucose (according to Lippincott´s Pharmacology, 2006
Comparison of Type 1 and Type 2 diabetes. (according to Lippincott´s Pharmacology, 4th ed., 2009)
Duration of non-insulin-dependent (type 2) diabetes mellitus, sufficiency of endogenous insulin, and recommended sequence of therapy Impaired glucose tolerance Normal Type II diabetes 5 – 15 years 0 – 5 years More than 15 years Relative ability to secrete insulin No treatment Diet Combina-tion therapy Multiple injections of insulin Diet plus sulfonyl-urea Increasing severity of disease (according to Lippincott´s Pharmacology, 2006)
INSULIN AND ITS ANALOGUESin DM treatment • Original sources of insulin – animal pancreatic tissue • Slightly different structure • Troubles with purity, allergic reactions, potency, Ab-formations • Not used anymore! • Nowadays only HUMAN insulins are used • Produced biotechnologically by recombinant technology in high purity • Human gene for insulin is being introduced into the E. Coli and its expression is stimulated • Insulin analogues • Producedbiotechnologically using recombinant technology • Several AA were changed in human insulin to alter its physico-chemical properties – esp. ability to dissociate from hexamer to monomer, which is absorbed • Specifically altered pharmacokinetic profile (absorption!!!) • Same pharmacodynamic as human insulin (equipotent)
Insulin and its analoguesRoute of administration/absorption • Parenteral route (injectables) • i.v. administration • Rather rare • Used only in emergency situations – mostly via infusions • Suitable only for soluble human insulin – regular! • Mainly s.c.!!! • Typically single dose administration (but s.c. infusion is also possible) • Different body areas and devices – topic for seminar • Rate of absorption determines onset of actions, drug concentrations and duration of action • Insulin hexamer, which is administered, must be dissociated to monomers to be absorbable • Rate of dissociation largely determines absorption and thereby onset and duration of clinical effect • i.m. also possible • less used, when more rapid onset needed
Insulin and its analogues Parenteral route (injectables) Factors having impact on drug absorption and onset/duration of action • site of injection • blood supply • temperature • physical activity
Alternative routes? • A chase for non-invasive insulin • Oral • common approach unfeasible – denaturation, digestion and/or poor absorption • Inhalation • Nanodispersed powder in gas • impractical inhalers • Efficacy issue • not better rather worse than standard insulin preparations • Safety issue – lung fibrosis or cancer? • Very expensive – poor cost-effectiveness • Future??? Pfizer discontinued production • Other routes are under evaluations
Insulin and its analoguesPharmacokinetics - DME • Distribution mainly into the extracellular volume • Insulin receptors are on cell membranes • Cannot cross membranes by passive diffusion • does not cross placenta to affect fetus • Vd=0.3 l/kg? • Metabolism/Elimination • more than 90% metabolic elimination – degraded by insulinases in the liver and kidney • less than 10% excretion in urine • Half-life of elimination is quite short (aprox. 10 minutes only) • Plasma concentration fluctuations (considerable intra- and inter-individual) complicate the situation
Insulin and its analoguesAdverse reactions • HYPOGLYCEMIA • Most frequent and important one • Symptoms: • sympathetic – nervousness, sweating, tremor, intense hunger, palpitation… • CNS related - speaking difficulties, weakness • Advanced CNS function impairment - confusion, drowsiness, changes in behavior, coma, and seizure. • Reasons: • Non-compliance - too high dose (or medication error), meal was not taken at the time, unexpected physical activity • Liver/kidney failure, infections etc. • Solution: sweet syrup or drink when patient is consciousness, otherwise glucagon i.m/s.c. or glucose sol i.v. • LIPODYSTROPHY, HYPERSENSITIVITY
Adverse effect observed with insulin (according to Lippincott´s Pharmacology, 2006
Insulin preparations • Rapid/ultra short-acting insulines • Insulin lispro, insulin aspart and insulin glulisine • Short-acting insulines • Regular insulin • Intermediate-acting insulines • Isophan (NPH) insulin • Long-acting • Glargine and detemir insulins • Pre-mixed preparations • lispro/NPH (e.g., 30/70%) • lispro/glargine etc…
Ultra short-actinginsulin analogues • Rapid onset and ultra short duration of action • Better stimulate prandial insulin secretion to avoid hyperglycemia • the lowest variability of absorption (approximately 5%) of all insulin • Possibility of more flexible treatment regimens • Risk of hypoglycemia (meal timing!) • Lispro • lysine/proline switch at the position 28/29 • More rapidly dissociate and is absorbed after s.c. admin. • Given 15 min before the meal to substitute postprandial insulin secretion • Aspart-substitution of the B28 proline with aspartic acid • Glulisine – double substitution • Similar profiles • Often combined with other insulin types
Short-actinginsulin • Regular insulin (Humulin R, Novolin R) • short-acting, soluble, crystalline zinc insulin • Usually s.c. (i.v. in emergencies – severe ketoacidosis) • rapidly decreases blood glucose • Effect - within 30 min; peaks between 2 - 3 hours after s.c. injection; lasts 5-8 hours • Should be injected 30-45 min before the meal to minimize the mismatching • the pharmacokinetics and pharmacodynamics of small doses of regular insulin differ greatly from those of large doses.
Intermediate-actinginsulin • Isophane (NPH) insulin suspension(Humulin N,. Novolin N): = Neutral protamine Hagedorn (NPH) insulin (also called isophane insulin) • Suspension of crystalline zinc insulin combined with polypeptide, protamine • Intermediate duration of action due to the delayed absorption of the insulin • complex with protamine is less-soluble • onset cca 2-5 hours; duration of 4-12 hours • Only s.c. (never i.v.). • Use in all forms of diabetes except diabetic ketoacidosis or emergency hyperglycemia • Usually given along with regular lispro, aspart, or glulisine insulin Given 2-4 times daily in patients with type 1 diabetes
Effect of subcutaneous administration of lispro insulin and regular insulin on (A) serum insulin concentrations, and (B) the rate of glucose infusion necessary to maintain normal blood glucose levels in 10 normal subjects. A – Serum insulin levels B – Rate of glucose infusion 120 450 Lispro insulin 400 100 Lispro insulin 350 80 Regular insulin 300 Serum insulin (U/ml) 250 Glucose infusion rate (mg/min) 60 200 Regular insulin 40 150 100 20 50 0 0 0 1 2 3 4 5 6 7 8 9 10 11 12 0 1 2 3 4 5 6 7 8 9 10 11 12 Hours Hours
Long-acting insulin analogues • Insulin glargine • Precipitation at the injection site prolonged absorption and longer action. • Slower onset than NPH insulin, (1-1.5 hours); maximum effect after 4-6 hours • flat, prolonged hypoglycemic effect (i.e., it has no peak). • This maximum activity is maintained for 11-24 hours or longer. • Must be given s.c. • Insulin detemir - Fatty-acid side chain attached - There is an increased propensity for selfagreggation after s.c. administration and reversible albumin binding - Properties similar to insulin glargine - Has the most reproducible effect of the intermediate- and long-acting insulins, and its use is associated with less hypoglycemia than NPH insulin. - Dose-dependent onset of 1-2 hours - Duration of action of more than 24 hours - Given twice daily to obtain a smooth background insulin level
Onset and duration of action of human insulin and insulin analogues. Aspart insulin, lispro insulin Glulisine insulin Regular insulin NPH insulin Extended zinc insulin Glargine insulin Relative plasma insulin level 0 6 12 18 24 Hours (according to Lippincott´s Pharmacology, 2006)
A. Effect of tight glucose control on hypoglycemic episodes in a population of patients receiving intensive or standard therapy. B. Effect of standard and intensive care on the long-term complications of diabetes. B A Many clinicians believe the increased risk of hypoglycemia that accompanies intensive therapy is justified by the substantial decrease in the incidence of long-term complications, such as diabetic retinopathy and nephropathy. Intensive therapy results in a three fold increase in the frequency of hypoglycemia. 100 Intensive therapy 60 Hypoglycemic episodes per 1000 patient months Standard Percentage of patients with complications Standard therapy 30 Intensive 0 0 0 1 2 3 4 5 6 7 8 9 (according to Lippincott´s Pharmacology, 2006) Year of study
Examples of two regimens that provide both prandial and basal insulin replacement. B = breakfast; L = lunch; S = supper A B Morning Afternoon Evening Night Morning Afternoon Evening Night Lispro Lispro Lispro Regular Regular Regular NPH NPH Insulin effect Insulin effect B L S Bedtime B L S Bedtime (according to Lippincott´s Pharmacology, 2006)
Mixtures Onset Peak Duration Humulin M3(30% regul. + 70% isophane) 30 min 1 – 9 h 14 – 15 h Novomix 70 (70% aspart + 30% protamine-aspart) 10 – 20 min 1 – 4 h 14 – 24 h Novomix 30 (30% aspart + 70% protamine-aspart)
Oral hypoglycemic agents (OHA) • Used in Type II DM only • why? • biguanides as the exception • Best response • in younger patients (around 40 years old) • in the first 5 years after onset • Advanced stage Type II DM may require • combination of oral hypoglycemic agents • combination with insulin (loss of β-cells due to the aging and disease)
Classification of OHAaccording to the mechanism of action • Insulin secretagogues • sulfonylureas (1st and 2nd generation) • meglitidines • Insulin senzitizers • biguanides • thiazolidindiones • Alpha-glucosidase inhibitors • acarbose • miglitol • Other agents - incretin mimetics - exenatide
OHA - Insulin secretagoguesI. Sulfonylureas • Promote insulin release from the β-cells • Additional effects ? • they reduce serum glucagon levels • they block K+ channels in extrapancreatic tissues • Mechanism of action • they bind to sulfonylurea receptor on ATP-sensitive K+ channels • binding of the drug make the channel close • depolarization opens Ca2+ channels, which drives the insulin exocytosis
OHA - Insulin secretagoguesI. Sulfonylureas • Pharmacokinetic aspects • oral administration • peak concentrations within 2-4 hours • high protein binding • cross placenta to fetus and enter mother's milk • contraindicated in pregnancy and lactation • liver metabolism may take place – metabolites can be active (glibenclamide, glimepiride) • excretion mainly by kidney (be careful in renal/hepatic failure) or liver • Duration of action • I. gen - 6-12h – tolbutamide - up to 60 hours – chlorpropamide! • II. gen - 10-24h • PK drug interactions – plasma protein binding and CYP interactions: NSAIDs, warfarin, IMAO, sulfonamides, chloramphenicol
OHA - Insulin secretagoguesI. Sulfonylureas • I. Generation • Tolbutamide • good absorption, but rapid hepatic metabolism • shorter duration of action • safe in elderly • devided dose • Chlorpropamide • very long half-life and duration of action • active metabolites • not safe in elderly (hypoglycemia is likely) • renal excretion (20-30% as unchanged)drug • consider renal function!!! • disulfiram-like effect, ADH-like effect, rare hematotox.
OHA - Insulin secretagoguesI. Sulfonylureas • II. Generation • More frequently prescribed • More potent, fewer adverse reactions, interactions... • Liver metabolisms – consider liver disease • glibenclamide (glyburide in USA) • avoid even in mild renal dysfunction – hypoglycemia is likely • glipizide • should be taken at least 30 min before breakfast (food slows absorption) • shorter half-life - lower risk of hypoglycemia • glimepiride • once daily administration (good compliance) • the most potent analogue
OHA - Insulin secretagoguesI. Sulfonylureas • Adverse effects • hypoglycemia • most frequent adverse reaction • consider - dose, patient's age, kidney/liver dysfunction, half-life of the drug, drug interactions • most often in chlorpropamide and glibenclamide • increased appetite and weight gain • insulin secretion-related effects • a trouble in obese patients with metabolic syndrome • GIT disturbances • disulfiram-like effects • they should by replaced with insulin for few days after MI
Oral Hypoglycaemic sulfonylurea drugs Duration of action and (half-life) In hours Drug Relative potency Pharmacokinetic aspects General comments A safe drug; least likely to cause hypoglycaemia May decrease iodide uptake by thyroid Contraindicated in liver failure Tolbutamide1 Some converted in liver to weakly active hydroxy- tolbutamide; some compound Renal excretion 6 – 12 (4) May cause hypogly- caemia. The active metabolite accumulates in renal failure Glibenclamide Some is oxidised in the liver to modetrately active products and is excreted in urine; 50% is excreted unchaged in the faeces 150 18 – 24 (10) 100 Glipizide May cause hypoglycaemia Has diuretic action Only inactive products accumulate in renal failure Peak plasma levels in 1 hour. Most is metabolised in the liver to inactive products, which are excreted in urine; 12% is excreted in faeces. 16 – 24 (7)
OHA - Insulin secretagoguesII. Meglitinides • repaglinide and nateglinide • mechanism of action as in SU drugs • more selective to β-cells than SU? • 2 binding sites on K+ channel • 1st same as for SU drugs, 2nd unique • Rapid onset and short duration of action • this is in contrast to SU drugs • postprandial glucose regulators • minimal effect on overnight or fasting glucose levels • administration shortly before meals • Often combined with – biguanides or thiazolidindiones
OHA - Insulin secretagoguesII. Meglitinides • Adverse reactions • hypoglycemia • less frequent, less severe than in SU • nateglinide • likely the lowest risk from all secretagogues • renal failure is usually not a trouble • liver dysfunction makes it more likely • weight gain • rather less than in SU • Drug interactions(CYP inhibitors/inducers) • repaglinide – metabolized by CYP3A4 • nateglinide - metabolized by CYP2C9 a 3A4
OHA- Insulin sensitizersI. Biguanides • Metformin • the only drug from this group used • phenformin – discontinued - risk of lactate acidosis • mechanism of action:complex and still not fully understood • reduces tissue insulin resistance • increases glucose uptake and utilization in the skeletal muscle • inhibits hepatic gluconeogenesis • slowing of intestinal absorption of glucose and stimulation of glycolysis in enterocytes • reduction of plasma glucagon levels • reduction of plasma LDL and VLDL • euglycemic effect rather than hypoglycemic
OHA- Insulin sensitizersI. Biguanides - metformin • Pharmacokinetics • not bound to plasma proteins • not metabolized • excreted by the kidney as the parent active compound • Clinical use • in obese type II DM patients • esp. in metabolic syndrome to overcome tissue resistance • administered usually once daily with breakfast • proven to reduce chronic complications • in combinations with secretagogues and thiazolidindiones
OHA- Insulin sensitizersI. Biguanides - metformin • Adverse reactions and toxicity • GIT disturbances • anorexia, nausea, vomiting, abdominal discomfort, diarrhea • the most frequent adverse reactions – in up to 20% patients • dose related • onset rather at the beginning – may be transient • vitamin B12 deficiency (decreased absorption) • lactate acidosis • rare but potentially fatal toxic effects • contraindication in: kidney/liver disease, alcoholism, hypoxic pulmonary disease, heart failure (predisposing factors) • NO HYPOGLYCEMIA – they are rather euglycemic agents
OHA- Insulin sensitizersII. Thiazolidindiones • Rosiglitazone, pioglitazone • Mechanism of action • agonists on PPAR-γ nuclear receptors • peroxisome proliferator-activated receptorγ • located in: adipocytes, myocytes, hepatocytes • modulate expression of genes involved in lipid and glucose metabolism, insulin signal transduction and adipocyte metabolism • reduce hepatic gluconeogensis • increase glucose uptake in the muscle/adipocytes • enhance effectiveness of both endogenous and exogenous insulin