Download
1 / 29
290 likes | 527 Vues
4.1. EMERGENCY HEALTH PROBLEMS AFTER DISASTERS. OFDA photo. PROBLEM 1: Disaster displaced populations, especially children, are particularly susceptible to five killer diseases. (< 5 years of age - 175 deaths). ARI/Pneumonia. Malnutrition. 23%. 9%. Malaria. 25%. Other. 22%.

E N D
4.1 EMERGENCY HEALTH PROBLEMS AFTER DISASTERS OFDA photo
PROBLEM 1: Disaster displaced populations, especially children, are particularly susceptible to five killer diseases (< 5 years of age - 175 deaths) ARI/Pneumonia Malnutrition 23% 9% Malaria 25% Other 22% Major Reported Causes of Death Children <5 Years, Refugee-Hosting Areas 9 Districts, July 1990 11% 10% Diarrhea Measles Source: UNHCR, MSF, ARC, IRC monthly report • InterWorks/UNHCR
BUT NOT ALWAYS - CONSIDER THESE CASES... NO excess mortality from NO excess mortality from communicable diseases communicable diseases Earthquakes in Turkey Earthquakes in Turkey n n Floods in Mozambique Floods in Mozambique n n Earthquake in El Salvador Earthquake in El Salvador n n Hurricane Mitch Hurricane Mitch n n World Trade Center World Trade Center Attack n n Papua New Guinea tsunami Papua New Guinea tsunami n n
Misconception about natural disasters and epidemics: Disasters do not introduce new diseases. Natural disasters are not always followed by epidemics.
Pneumonia 3% Cancer 3% Cardiovascular 10% Other 16% Physical Trauma e.g. violence Cause of Death all ages Sarajevo, Bosnia 1992-93 MSF
Cause of Death of those age >4 IRC Kelamie 2000
Problem 2:Managers and health specialists do not adequately understand the overall health situation of large, moving or displaced populations. Curative, clinical care is believed by many to be the first and dominant priority in all emergencies. It’s not. Rarely is it even a high priority. UNHCR photo
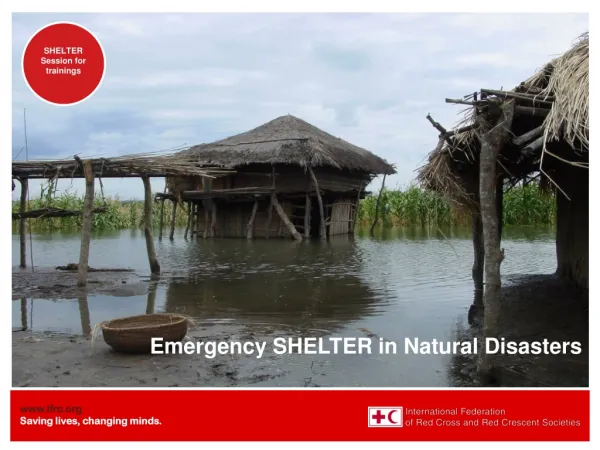
Problem 3: Other key sectors are not adequately addressed, resulting in serious public health threats ,ultimately requiring curative health response UNHCR photo/R. Darolle: Kao I Dang refugee camp, 1983
Problem 4: Diarrheas can become deadly in mass displacement scenarios. UNHCR photo, H.J. Davies, - Cholera and other water-borne diseases claimed up to 3,000 live a day in late July 1994, Goma, Zaire
What is a diarrhea? • We can’t begin to identify the pathogen, which could be any number of viruses, bacteria or functional (or genetic) abnormalities. • We use an operational definition of 3 or more watery stools per day • Note: most rural young children in most poor countries have diarrhea 20 or more times per year.
MCH clinic reporting, Children Kabul Afghanistan 1997
Dysentery: 3 or more liquid stools per day with blood
Faryab Province, Afghanistan 2001 Famine and IDP by Save US CMR of 2.6/10,000/day reported
Faryab Province, Afghanistan 2001 Famine and IDP by Save US CMR of 2.6/10,000/day reported Malnutrition
Cholera • Severe profuse watery diarrhea with or without vomiting • Will kill quickly if not properly addressed… rehydration • 1 out of 10 infections becomes a case. • 1 out of 10 cases may die. MSF photo
IV drip treatment of cholera victims at a refugee camp in Mozambique.[Medecins Sans Frontiers/Doctors Without Borders photo]
Problem 5:Lack of organization in health programs and lack of communication with other sectors and among agencies results in imminent health threats. Malnutrition, resulting from lack of adequate food, water and sanitation ultimately results in the need for curative medical response
Problem 6: Lack of consultation with the refugee population—and women in particular—results in health services not reaching those in need and corresponding negative health consequences BBC photo
Problem 7: Overcrowding and lack of vaccination coverage result in life-threatening epidemic outbreaks of otherwise easily controlled diseases Jalozai refugee camp , Aug. 2001
Problem 8: Health (and other) programs begin too late. epidemiologic survey in the Gode district of Ethiopia, the center of the famine in the Somali region that began in 1999,
“In this epidemiologic survey in the Gode district of Ethiopia, the center of the famine in the Somali region that began in 1999, Salama and colleagues found that most of the 293 deaths during the famine were due to wasting and communicable diseases, including 47 potentially preventable measles-related deaths among children aged 14 years or younger. Approximately 77% of the deaths occurred before the major humanitarian relief interventions began in April/May 2000.” From: JAMA Vol. 286 No. 5, August 1, 2001
Problem 9:Delayed implementation of priority health measures, including surveillance, results in excess morbidity and mortality MSF photo – cholera ward - Bangladesh
Death Rate Calculation Deaths/10,000/day = Number of deaths x 10,000 Days counted x population So… If 21 people have died in one week out of a total population of 5,000, then what is the death rate?
Death Rate Calculation Number of deaths x 10,000 Days counted x population 21 (deaths) x 10,000 7 (days) x 5,000 (total pop.) or 6/10,000/day Is that good, acceptable, or bad? Why?
PROBLEM 10: Inappropriate or inadequate health programs result in higher than necessary rates of morbidity and mortality
OK 53 (deaths) x 10,000 90 (days) x (total pop. under 5) 60 people have died in a population of 20,000 in the last three months. What is the death rate, and what does it mean? 60 (deaths) x 10,000 90 (days) x 20,000 (total pop.) = 0.33 On further analysis of the data, 53 of these deaths were children under age 5, how would you report this finding and what does it tell you?
This is the age profile of the population TOTAL POPULATION IS 20,000 +13% < 5 = 2,600 people +12% 5 - < 15 = 2,400 people +15% 15 - < 20 = 3,000 people +52% 20- < 60 =10,400 people + 8% 60 + = 1,600 people = 100% =20,000 people How do you determine the <5 MR?
53 (deaths of children<5) x 10,000 90 (days) x (2,600 children<5) = 2.3 What types of bias may be present in the CMR and <5 MR? How might thes biases be addressed? How much assessment detail is needed in emergency response situations where time is of the essence? Now review the short paper: “Mullahs, Mountain Tops, and Mortality: Creative Demography in Refugee Emergencies”
CONCLUSION: • Health problems vary with disaster type and cause. • For emergency settlements in crowded conditions, pubic health concerns relate primarily to epidemic disease outbreaks. • Public health concerns are almost always best solved by provision of basic services. • Failure to meet standards in food, nutrition, shelter, water and sanitation sectors will lead to significant health problems and excess mortality.