Expenditure on CVD
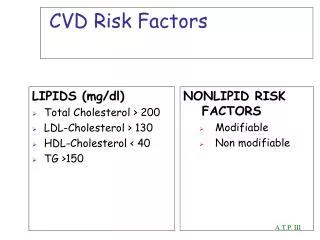
Expenditure on CVD. Inequity? Orientation of services: Treatment versus prevention. Cost impacts of CVD. Direct financial costs to the Australian health system Other (indirect) financial costs including Productivity losses Carer costs Deadweight loss from transfers

Expenditure on CVD
E N D
Presentation Transcript
Expenditure on CVD Inequity? Orientation of services: Treatment versus prevention
Cost impacts of CVD • Direct financialcosts to the Australian health system • Other (indirect) financial costs including • Productivity losses • Carer costs • Deadweight loss from transfers • Other costs – aids, equipment, transport and accommodation etc. • Non-financial costs – Burden of Disease • Value of Statistical Life • Disability, loss of wellbeing and premature death • Measured in Disability Adjusted Life Years (DALYs) • Different costs of CVD are borne by different economic entities
Economic burden of CVD in 2008 • CVD one of the biggest health burdens in Australia Estimated total $162 billion • ↑ of 71.4% compared with cost in 2005 • $13.1 billion in financial costs • $148.9 billion non-financial costs Access Economics Pty Ltd. The growing cost of obesity in 2008: three years on. August 2008
Health care expenditure • Government funded almost 70% of health expenditure in 2007-08 • Recurrent expenditures on health in 2007-08 included: • Hospital services (39.3%) • Medical services (18.7%) • Benefit-paid pharmaceuticals (14%) – excluding those dispensed in hospitals AIHW. Australia's health 2010. 2010
CVD accounted for the greatest amount of government expenditure (11%) in 2004-051 AIHW. Australia's health 2010. 2010.
Expenditure: Treatment vs prevention • 2.2% of governments’ total recurrent expenditure was spent on public health in 2007-08 • ↑ of 2.0% since 2006-07 • largely due to ↑ spending on immunisation programs AIHW. Australia's health 2010. 2010.
Public health expenditure 2007-08 AIHW. Australia's health 2010. 2010.
Indigenous groups • A study by Vos et al. (2007) found ATSIP suffer an overall burden of disease 2.5x that of the total Australian population • 2/3 of health gap was due to mortality and 1/3 due to disability • 70% health gap due to chronic diseases including CVD • AIHW: The Health and Welfare of Australia’s Aboriginal & Torres Strait Islander Peoples. 2005 AIHW. Australia's health 2010. 2010
ACE-Prevention - Assessing Cost-Effectiveness in Prevention (Sept 2010)http://www.sph.uq.edu.au/bodce-ace-prevention • National Health and Medical Research Council funding • Supported by the Cooperative Research Centre for Aboriginal Health. • ACE Prevention Report • Recommendations to support more spending on prevention • Analysis of the value of many health advancement strategies to address the burden of preventable death and disease in Australia. • Efficient + fairer system of health
Main findings: Large impact on population health (i.e. >100,000 DALYs prevented per intervention): • taxation of tobacco, alcohol and unhealthy foods; • a mandatory limit on salt in just three basic food items (bread, cereals and margarine); • using an absolute risk approach • using cost-effective generic drugs (low-cost polypill = 3 BP-lowering + 1 cholesterol-lowering) • gastric banding for severe obesity
Main findings: Moderate impact on population health (10,000 to 100,000 DALYs prevented per intervention): • screening programs for pre-diabetes, CKD and low bone mineral density in elderly women. • drug and lifestyle treatments recommended for the high-risk individuals identified by such screening programs. • smoking cessation aids, pedometers and mass media for physical activity
Dominant interventions • The package of 20 ‘dominant’ interventions could avert one million DALYs over the lifetime of the 2003 Australian population. • 80% of this health gain could be achieved with the taxation and regulation interventions on salt, alcohol and tobacco, and the polypill for CVD prevention. • Cost = $4.6 billion, • Savings = $11 billion in health care costs