CVD Workshop
CVD Workshop. SDPI CVD Risk Reduction Project Meeting #5 Denver, Colorado. Case Study. 62 year old woman presents for her scheduled intake visit for your CVD project She has been overweight most of her adult life and has a BMI of ~32 PMHx: HTN, diet controlled diabetes

CVD Workshop
E N D
Presentation Transcript
CVD Workshop SDPI CVD Risk Reduction Project Meeting #5 Denver, Colorado
Case Study • 62 year old woman presents for her scheduled intake visit for your CVD project • She has been overweight most of her adult life and has a BMI of ~32 • PMHx: HTN, diet controlled diabetes • Medication: HCTZ 25 mg Q day
Case Study • SHx: Walks to the bus every day and occasionally walks with friend on the weekend • She smoked ½ pack/day until 2 years ago • FHx: Her sister is overweight, and take metformin for diabetes, her father died from a heart attack, her mother has diabetes
Case Study: Physical Exam • Vitals: Height: 64” Weight: 188 lb BP 140/90 Waist Circumference: 39” • Exam: HEENT WNL, Lungs clear, Heart RRR S1/S2 no murmur, GI obese abdomen, Foot exam: monofilament normal in both feet, pulse and skin normal, no pedal edema, nails mild fungal changes
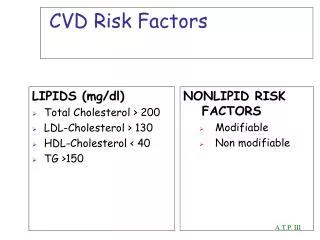
Case Study: Initial Laboratory • FBS: 165 mg/dl, • A1c 8.1% • TC: 220 mg/dl • TG: 240 mg/dl • HDL-C: 38 mg/dl • LDL-C: 134 mg/dl • Creatinine: 0.6 mg/dl • Urine M/C Ratio: 35
Modifiable Major Risk Factors Hypertension Hypercholesterolemia Smoking Microalbuminurea Hyperglycemia Contributing Causes Obesity, fat distribution Lack of physical exercise Genetic factors Age Disease duration Cardiovascular Risk Assessment: Garber, AJ American Family Practice December 15 2000
0 -10 -20 -30 -40 -50 United Kingdom Prospective DiabetesStudy (UKPDS): Results BP Control (144/82 vs 154/87 mm Hg) Glucose Control Any diabetes- related endpoint Any diabetes- related endpoint Micro- vascular endpoints Diabetes- related death Diabetes- related death Micro-vascular endpoints Stroke -10% (P=.34) -12% (P<.0001) -25% (P<.005) -25% (P<.01) -32% (P=.019) -37% (P=.009) -44% (P=.013) UK Prospective Diabetes Study Group 38. BMJ. 1998;317:703-713. UK Prospective Diabetes Study Group 33. Lancet. 1998;352:837-853.
STENO-2 Study:Multifactorial Intervention and CVD in Patients with Type 2 Diabetes • Denmark Study: NEJM 1/30/2003 • 160 patients with type 2 diabetes • 8 year study with mean age 55 years • Two study groups: intensive therapy and conventional therapy Gaede P, et al. N Eng J Med. 2003;348:383-393.
STENO-2 Study:Multifactorial Intervention and CVD in Patients with Type 2 Diabetes • Intensive Group: stepwise implementation of behavior modification and pharmacologic therapy targeting: • Hyperglycemia • Hypertension • Dyslipidemia • Microalbuminurea Gaede P, et al. N Eng J Med. 2003;348:383-393.
STENO-2 Study:Multifactorial Intervention and CVD in Patients with Type 2 Diabetes • End point: • Death from cardiovascular causes • Nonfatal myocardial infarction • Stroke • Coronary or peripheral artery revascularization • Amputation as a result of ischemia Gaede P, et al. N Eng J Med. 2003;348:383-393.
STENO-2 Study:Multifactorial Intervention and CVD in Patients with Type 2 Diabetes Macrovascular Complications • Conventional Group: 44% of patient had a primary end point event • Intensive Group: 24% of patients had a primary end point event Primary composite endpoint: Death from CV causes, nonfatal MI, CABG, PCI, nonfatal stroke, amputation, or surgery for peripheral atherosclerotic artery disease. Adapted from Gaede P, et al. N Eng J Med. 2003;348:383-393.
Intensive Multiple Risk Factor Management Patients with Type 2 Diabetes and Macroalbuminuria 60 N=160; follow-up=7.8 years Conventional Therapy 20% Absolute Risk Reduction 40 Primary Composite Endpoint* (%) 20 • Aggressive treatment of†: • Microalbuminuria with • ACEIs, ARBs, or combination • Hypertension • Hyperglycemia • Dyslipidemia • Secondary prevention of CVD Intensive Therapy† 12 24 36 48 60 72 84 96 Months of Follow-Up Primary composite endpoint: conventional therapy (44%) and intensive therapy (24%). *Death from CV causes, nonfatal MI, CABG, PCI, nonfatal stroke, amputation, or surgery for peripheral atherosclerotic artery disease. †Behavior modification and pharmacologic therapy. Adapted from Gaede P, et al. N Eng J Med. 2003;348:383-393.
Smoking Cessation Hyperglycemia CVD Risk Reduction Lifestyle Changes Weight loss, healthy foods, Increased activity Daily Aspirin Lipid Control Hypertension Control
JNC 7 “Failure to titrate or combine medications, despite knowing the patient is not at goal BP, represents clinical inertia and must be overcome.” Chobanian A, et al. JAMA. 2003;289:2560-2572.
Treatment of Hypertension in Diabetes Diagnosis of Hypertension BP>130/80 mm Hg Non-Pharmacologic Therapies Drug Therapies ACE based regimes preferred Multi-drug therapy often needed Target BP <130/85
Step-wise progression to controlling Blood pressure ACE & ARBS Limits nephropathy and Lower CVD risk Blocker Ca++CB Thiazide -Blocker*
Average Number of Antihypertensive Agents Needed Per Patient to Achieve Target BP Trail Target BP mm Hg Number of Antihypertensive Agents UKPDS DBP<85 ABCD DBP<75 VDRD MAP<92 HOT DBP<80 AASK MAP<92
SUMMARYTreatment of Hypertension in Diabetes • Blood pressure goal in diabetes = 130/85 • Level of blood pressure more important that type of therapy • Reduces rates of both micro and macrovascular disease • ACE based therapies: 1st Line Choice • Reduces CVD complication and offers reno-protection • Multi-drug therapy often needed • Aggressive treat essential, if CVD and renal disease present ideal goal: 125/80 (?) Arch Intern Med, Vol160, Sep 11, 2000, 2447-2452
Prevalence of Dyslipidemia in Type 2 Diabetes • Most common pattern is elevated triglycerides and low HDL • TC & LDL concentration is often the same as non-diabetic individuals • However, LDL particles are smaller, denser and more atherogenic
Goals for Control • LDL < 100 • HDL> 45* in men, HDL> 55 in women • Lipid panel annually • Consider direct LDL if TG >250 or if specimen is non-fasting • All patients with LDL > 100 need medical, dietary and lifestyle intervention
Considerations in Therapy • Diet and exercise are key • Hyperglycemia itself will lead to increased TG: try to improve sugars first • Metformin will decrease LDL • Glitazones will decrease TG, increase HDL • Check TFTs in initial work-up • Metamucil, increased dietary fiber
Microalbuminuria and Diabetes • Independent risk factor for development of cardiovascular disease • Predictor of cardiovascular mortality in the diabetic population • Part of the cardiometabolic syndrome
Microalbuminuria and Diabetes • Test for urine protein yearly • If negative, screen for microalbuminurea • Dipstick + microalbuminurea should be confirmed on a separate specimen • A/C ratio: 30mg/gm • Treat with ACE-inhibitor, regardless of BP
Smoking Cessation • Smoking doubles the risk of CVD in patients with diabetes • Attenuates the benefit of gained from modifying other risks • Synergistic with TC, possibly through enhanced oxidation of LDL • MRFIT: independent and ing risk of CVD based on #cigarettes/day
Smoking Cessation: Standards of Care • Assessment of smoking status and history • Counseling on smoking prevention and cessation • Referral to program for delivery of smoking cessation
Aspirin Therapy in Diabetes “Aspirin - the poor man’s statin” • Reduces risk of MI by ~ 15-60% • Treat all high risk patients with diabetes over the age of 35 • Use 81 – 325mg/day The Lancet
Procoagulant State • Platelets are overly sensitive to platelet aggregating agents • High levels of Thromboxane, a potent vasoconstrictor • Decreased fibrinolytic activity • Increased levels of Plasminogen Activitor Inhibitor-1 • Clot lysis cannot precede normally
Goals for treatment Primary Prevention: • Strongly consider ASA in patients > 30 with diabetes and high risk for CVD • FHx CVD, smoking, HTN, obese, albuminurea, dyslipidemia Secondary Prevention: • ASA for patients with know CVD: MI, stroke, PVD, claudication, angina DOSE: 162mg to 325mg
Conclusion: Aggressive modification of all identified CVD risks factor is essential to reduce the macrovascular complications of diabetes