Download
1 / 61
610 likes | 900 Vues
Regulating Drug Prices with Ramsey Pricing Principles. Robert Kemp, PhD (Econ) Associate Professor College of Pharmacy, Touro University. College of Pharmacy Touro University-California. 1. Regulating Drug Prices with Ramsey Pricing Principles. Introduction.

E N D
Regulating Drug Prices with Ramsey Pricing Principles Robert Kemp, PhD (Econ) Associate Professor College of Pharmacy, Touro University
1. Regulating Drug Prices with Ramsey Pricing Principles Introduction
Regulating Drug Prices with Ramsey Pricing Principles • Introduction • Regulation of pharmaceuticals • Ramsey optimality • Ramsey principles for price setting • Conclusion • Appendix (Cost-effectiveness analysis cannot and should not be used to set prices.)
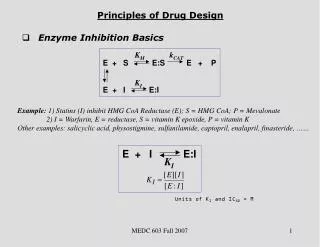
II. Regulation of Pharmaceuticals • Regulation of which drugs can be prescribed; marketing regulation. • Regulation of prescribing practice. • Determination of expenditures in a therapeutic area, i.e. anti-diabetic agents. • Determination of price ceilings. • Determination of level of reimbursement or subsidy.
Institutional settings for health economics decisions affecting drugs • Allocation of resources among providers • Insurance • Medical care • Hospitals • Pharmaceuticals • Allocation of resources among therapeutic areas or disease states. • Allocation of resources by controlling access to drugs in a therapeutic area. • Allocation of resources by controlling price for pharmaceuticals within a therapeutic area.
Regulating Drug Prices • Prices of drugs are regulated in many countries, including the USA. The methods include • Reference pricing, ceiling prices, subsidization, rate of return, “AMP+FUL”, “Best price”, etc. • There are also restrictions that affect level of reimbursement or access • Clinical recommendations, prior authorization, and other administrative rules. • Cost-effectiveness analysis or another form of economic evaluation (programme evaluation) threshold
Economic efficiency • None of the rules of administration seem to be based on economic efficiency criteria, or microeconomic principles. • The relationship between economic evaluation and pricing is not stately explicitly. • Ramsey pricing, or the inverse elasticity rule, has been suggested (and sometimes institutionalized) as the rationale for pricing in many industries including the pharmaceutical industry.
Ramsey Price Regulation • As a guiding principle or “Rule of Reason” • Microeconomics replaces regulatory precedent as foundation of regulation. In 1970’s economists showed the inefficiency of existing price regulations in transportation, energy, public utilities, and other industries. • New insights into sustainability of monopoly, optimal departures from marginal cost pricing, optimal commodity taxation, and multi-part pricing, etc. • Principles of marginalist approach were widely accepted but few attempts to base positive regulatory approach to assure performance under regulation. “Informational constraints” the usual reason cited for not pursuing Ramsey optimality as new “rule of reason”.
Regulating Drug Prices with Ramsey Pricing Principles I • Hypothesis I: • If there was a monopsonist who wanted to set prices on drugs for a population within a therapeutic area, then using Ramsey principles would be an improvement over economic evaluation techniques and over capricious administrative decisions based on some notion of cost-containment or solely on the basis of clinical effectiveness.
Regulating Drug Prices with Ramsey Pricing Principles II • Hypothesis II: • If there was a monopsonist who wanted to set prices on drugs for a population across therapeutic areas, then using Ramsey principles would be an improvement over economic evaluation techniques, and over capricious administrative decisions based on some notion of cost-containment, or solely on the basis of clinical effectiveness.
Price regulation of pharmaceuticals • Relevant market to be considered for pricing • Population in a Geographic area • Therapeutic area (examples diabetes, hypertension) or disease state. • Should regulate relative prices within the market and not worry about so called “silo effects”.
Normative goals through pricing • For pharmaceutical companies • Innovation: New drugs that are “priority NMEs” are given higher prices (or higher subsidies). • Reward for performance: A drug that produces better outcomes in a therapeutic area is given higher prices. (Is this reflected in elasticity of demand?) • Costs can never be used as sole justification of prices, however prices need to reflect the long-run average costs of drug companies.
Normative goals through pricing • For health authority or third-party payer • Deadweight loss due to monopoly is minimized: agencies assign second-best prices on drug commodities. • Deadweight loss due to monopsony is minimized: agencies assign optimal taxes on drug commodities (subsidies are negative taxes). • Payers act as financial agent of the patient insuring that patients are given access to the drugs that improve their health. (Play volume game.)
Normative goals through pricing • Preserve the clinical imperative: Medical expert (clinical agents) look after patients insuring that patients are given access to the drugs that improve their health. • Relate the evaluation of clinical effectiveness and the differential prices of drugs in a therapeutic area. • (Consumers get the drugs they are willing to pay for?)
Ramsey Pricing • For simplicity, suppose that the demand functions for the n produced drugs in a therapeutic area (q1, q2, ..., qn) are independent: • qi = Di(pi), for i = 1, 2, ..., n. • The total revenue available for the drugs is • R(q1, ..., qn) = p1(q1)q1 + ... + pn(qn)qn.
Ramsey Pricing The cost of producing these goods is C(q1, ..., qn). The regulator wants to choose outputs so as to maximize consumer surplus, qi 0 pi(t)dt - C(q1, ..., qn),
Ramsey Pricing subject to the constraint that revenue exactly equals cost (or that profit is a given constant). The first-order conditions are pi - Ci = ג(Ri - Ci) for i = 1,... ,n, where Ci and Ri are the partial derivatives of C and R with respect to qi and גis the Lagrangian multiplier on the constraint.
Ramsey Pricing This condition may be rewritten as pi – Ci ki pi εi = where k = ג /(1 + ג) and εiis the elasticity of demand for qi. That is, the price markup over marginal cost, (pi - Ci)/pi, is inversely proportional to the price elasticity of demand for that good. If k = 1, this condition is the standard monopoly price-discrimination condition. If k = 0, this condition is the same as in competition.
Ramsey Pricing • Ramsey Pricing is "second-best" pricing, whereby drugs for patients with inelastic demands pay a higher markup over marginal cost than those with more elastic demands. • The basic goal of Ramsey Pricing is to recoup the fixed costs from those patients who have the fewest alternatives, while minimizing the distortion associated with prices in excess of marginal costs.
Ramsey Prices and Taxes • In order for the rules of optimal relative prices and optimal taxes to be applied, we must set out a price for one good as a “numeraire” upon which all other relative prices are set. • This is the major normative decision to make.
Where do you get the εi ? • Based on clinical imperative? • from prescribers preference and derivation of an index based the order preference of expert medical doctors? • based on a combination of epidemiology, best practice, evidence-based medicine, clinical effectiveness? • Utility values? • Based on consumers willingness to pay? • Based on expenditure cap in a therapeutic area?
Price Regulation of Drugs • Where do you get the Ci? • In other industries prescriptive accounting rules are used with an attempt to find long-run MC (Kahn, Baumol). • Cost should capture relevant R&D costs, so that priority NME’s are rewarded. • Majority of marginal costs in USA are marketing costs.
2004 Revenue Allocation for Top 7 US Pharmaceutical Cos Marketing, Advertising and Administration Other 32% 36% 14% 18% Research & Development Profits (net income) Source: Families USA, The Choice: Health Care for People or Drug Industry Profits, 2005
Price Regulation of Drugs • What about the budget (or profit) constraint? • Set it arbitrarily to company at industry average in fully allocated model (like in UK). • Effectively, the amount allocated to a therapeutic area from a monopsonist will determine the revenue that can be taken from the market by a particular company for a particular drug.
Initial pricing • The most important use of Ramsey principals maybe in setting the initial price upon entry. • There is evidence of inherent inverse elasticity in pricing.
Me-toos • Entry of a me-too into a market would increase ε for both the incumbent product and the rival entrant.
Set prices on a yearly basis • Ex ante price for new drugs based on clinical outcomes and doctor’s preferences. • Ex post review of existing drugs (like France). • Econometric test for Ramsey optimality in existing pricing structure. • (Ramsey-like monopolistic price discrimination was found in rail prices in sustainably monopolized markets prior to rail price regulation (Dumas, “Weak Invisible Hand”). In postal prices prior to entry by other carriers.)
What about generics? • In theory, Ramsey optimality conditions hold as monopoly goes to rivalry, or competition through entry. (see Breutigam,1984, or Miller, 2007). • (As k becomes zero, we approach a competitive solution where p = MC.)
Subsidy or price regulation? • What about supply induced demand? • With a monopsonist and a patented monopoly it doesn’t matter whether you use Ramsey optimal taxes (subsidies) or Ramsey optimal prices. There is no difference between a price regulation and a tax in this case (Baumol and Bradford, 1970).
Ramsey optimal pricing across therapeutic areas • Ramsey optimality is sustained across a class of firms with different elasticities and cost structures that provide the same output, known as the “intra-modal case” taken from transportation pricing. • Once one has a numeraire price in one market, relative prices (optimal) within a market and relative prices (optimal) across modes can be found.
Conclusion • Ramsey optimality can be used to set a “rule of reason”; or the theoretical foundation for drug prices in a therapeutic area. • “Informational problems” will exist in an attempt to institutionalize the rule of reason, however, having an efficiency criteria guiding pricing may lead to improvements in allocation over existing administrative rules.
Ramsey Optimality • Ramsey optimality can be set up to give the essential relationship between the value of the drug therapy to the patient and the optimal prices. Such a valuation of output can be based on expert clinical imperative, community-based values (utilities), or WTP. • Costs can be explicitly assigned by the monopsonist, and can take into account the effect of the adaptation of new technologies on capital cost.
Ramsey Optimality • Programme evaluation techniques assume that prices are exogenous to the evaluation and should not be used to set prices. • Clinical imperative should be preserved: Outcome afforded by the technology is substantiated on clinical grounds and built into the pricing regulation. • Ramsey optimality does not have the artificial disjoint between a “budget impact” analysis and cost-effectiveness analysis. • The “margin” for which “incremental CEA” is targeted is often undefined. The Ramsey optimal formulation begins with a budgetary constraint and so defines the optimality conditions.
Ramsey optimal commodity taxes • Model of single buyer (monopsonist) • Goal is to find the least-distorting pattern of taxes • Assumes infinite supply elasticity • Results: • optimal taxes vary between goods such that tax rates are proportional to the elasticity of demand • Reduces compensated quantity demanded for each good by the same percentage relative to pre-tax demands • Baumol and Bradford (1970) show that Ramsey rule is equivalent to inverse elasticity rule for monopolist if there are no cross price effects
Average Investment per Stage of DevelopmentPer Compound Including Failures 250 175 $Millions 51 33 31 Note: Does not include Capital Investments, Time Value of Money, or Risk Free Return on Capital. Source: IMS Internal Analysis
Average Investment for Stage of DevelopmentPer Compound Excluding Failures 33 $Millions 14 11 5 5 Note: Does not include Capital Investments, Time Value of Money, or Risk Free Return on Capital. Source: IMS Internal Analysis
Revenue from Blockbuster RX Millions US$ Patent years after launch Years off patent
Prescriptions of Blockbuster RX Prescriptions 1,000 Patent years after launch Years off patent
NCE Lifecycle Sales AnalysisAverage Percent of Peak Sales Potential Hatch Waxman Exclusivity Source: IMS (Based on 816 NCE’s launched since 1983)