Download
1 / 17
220 likes | 586 Vues
Obesity and Endocrine Disorders. Dr EM Selepe MBChB (Natal ) FCA(SA) 1 Military Hospital Thaba Tshwane. Obesity Definition. Excess of body fat sufficient to adversely affect health BMI is used as the surrogate marker Obesity is often defined in terms of the BMI

E N D
Obesity and Endocrine Disorders Dr EM Selepe MBChB(Natal) FCA(SA) 1 Military Hospital Thaba Tshwane
Obesity Definition • Excess of body fat sufficient to adversely affect health • BMI is used as the surrogate marker • Obesity is often defined in terms of the BMI • BMI does not take body build into consideration and hence can be misleading in the presence of large muscle mass • Fat distribution can be central (abdominal) or gluteo-femoral • Central obesity has increased CVS risk factors
Obesity Assessment • BMI commonly used • Waist to hip circumference ratio (WHR) can be used or waist circumference alone • Using BMI Wt/Ht squared (kg/m2) • WHO classification: • <18,5 Underweight • 18.5 - 24.9 Healthy • 25 – 29.9 Overweight • 30 – 39 Obese • >40 Morbid Obesity
Obesity Assessment“Cont” • WHR (waist to hip ratio) • Male >1.0 Female >0.9 • Waist circum Male> 103cm and female >88 cm • Generally Waist < 100cm suggests insulin resistance less likely in all sexes
Epidemiology • Rapid increase in both developed and developing countries • Prevalence on the increase stats from the UK: • 1980 6% of male and 8% of female • 2000 increase to 21% and 21.4% respectively • Now 55% of population is overweight or obese
Clinical Problems • Psycho-social: • Poor self esteemand image • Depression • Withdrawn • Medical: • Gastro-oesophageal disease (GED) • Secondary hypertension • Pulmonary hypertension • Obstructive sleep apnoea (OSA)
Anaesthetic Practice • Upper airway • Short neck, neck circumference (male 42cm , female 41cm) • Fat padding • Large face- difficulty in holding mask • Mallampati grades 3 to 4, Thyromental <6cm and sternomental < 12cm distance • Poor mouth opening
Anaesthetic Practice“cont” • Lower Airway: • Poor lung compliance • Increased airway resistance – chest bulk • Higher peak airway pressures • Pulmonary hypertension • Decreased FRC leading to atelectasis and hypoxia • Increased abdominal pressure decreasing the FRC ( Functional residual capacity )
Anaesthetic Practice“Cont” • Cardio-vascular System: • Secondary hypertension • LVH, LAH leading to diastolic dysfunction • RVH from pulmonary hypertension leading to RHF • Prone to DVT and pulmonary thromboembolism – worsening pulmonary HPT • OSA leads to hypercapnia, sympathetic over stimulation worsening pulmonary and systemic hypertension .
Anaesthetic practice “cont” • GIT • Gastric emptying- delyed, potential full stomach • Gastroeosophageal disease ( reflux) • Associated disease ( hiatus hernia) • Pressure on the splanchnic vessels compromises liver perfusion.
Anaesthetic considerations Anticipated problems: • Airway management • Potential full stomach ( starvation period prolonged , ulcer prophylaxis ) • Positioning of patient and intravenous access • Co - morbid diseases • Possible post op high care or ICU – OSA • Deep venous thrombosis prophylaxis
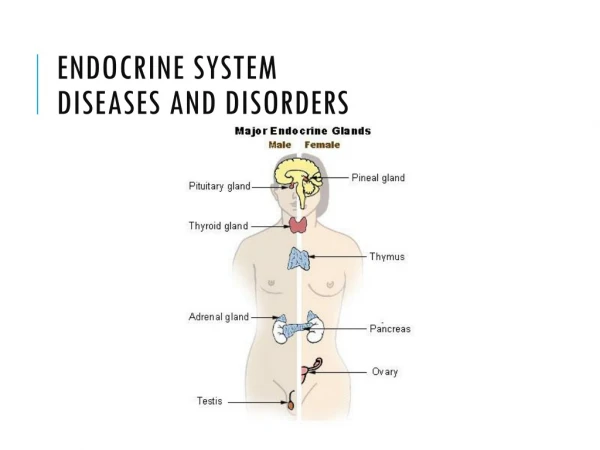
Endocrine Disorders( Metabolic Syndrome ) • Components • > Waist circumference • Increased insulin resistance ( Diabetesmellitus) • high LDL , decreased HDL • Hypertension
Diabetes mellitus and Obesity • There is increased incidence of obesity and Diabetes • Obese patients have increased resistance to insulin. • Type 2 diabetes is common in these population • Commonly on oral hypoglycaemics and or insulin.
Aims of Treatment • Sensitize receptors (thiazolidinediones , Biguanides ) • Increases the B cells production of insulin( sulphonylurea , Biguanides , GLP I (glucagon like peptide 1) ) • Decrease absorption (alpha1 gylcosidaseinhibitors) • Insulin replacement
Anaesthetic considerations • Uncontrolled DM • Dehydration (polyuria , polydypsia) • Hyperosmolality (HONK) • Sepsis • Chronic DM • Potential full stomach • Autonomic and peripheral neuropathy • Coronary artery diseases and HPT • Kidney dysfunction/failure
Conclusion • There is an accelerated prevalence of obesity and diabetes mellitus in South Africa and knowledge of the two entities is of essence as it is also part of metabolic syndrome. • Airway management and the clinical dynamics of the two should be well appreciated.