Download
1 / 19
340 likes | 1.15k Vues
DIABETES AND INSULIN RESISTANCE. KARI KOHRS RD LDN CDE UICMC NUTRITION & WELLNESS CENTER . DIABETES PREVALANCE. Third leading cause of death-- United States 18 million diagnosed Growing at the rate of 3 new cases q 2 mins

E N D
DIABETES AND INSULIN RESISTANCE KARI KOHRS RD LDN CDE UICMC NUTRITION & WELLNESS CENTER
DIABETES PREVALANCE • Third leading cause of death-- United States • 18 million diagnosed • Growing at the rate of 3 new cases q 2 mins • Alarming incidence of type 2 DM • 18 yr old and younger type 2 DM skyrocking
THE OBESITY PROBLEM • 80% of Type 2 DM are overweight • Particular forms of obesity-- • Abdominal • Truncal • Visceral • Subcutaneous • Central body obesity and insulin resistance are related--releases more FFA • Insulin resistance has 2 causes-high levels of circulating fat and inheritance
Causes & Aggravating Factors of Insulin Resistance • Combination of genetic and lifestyle factors • Heredity--close relatives with Type 2 risk • Ethnic group--Native Americans, AA, Hispanics • Abdominal obesity interferes w/ insulin action • Lack of exercise and high caloric diet • Stressful lifestyle—stress hormones released • Pregnancy-increase in weight and production of placental hormones that blood glucose levels
The body RESISTS taking sugar into the cells Insulin can’t link with the receptors on the surfaces of cells because there aren’t enough receptors Something goes wrong in the chemical reaction at the time of linking The body can’t use the sugar in the blood & hi BG develops bringing on DM symptoms Certain proteins and/or enzymes released by stored fat act on muscle and liver cells to impair the way they “read” insulin signals to process glucose Visceral abdominal fat sheds more free fatty acids; elevated TG levels increases insulin production promoting further fat storage INSULIN RESISTANCE DEFINED
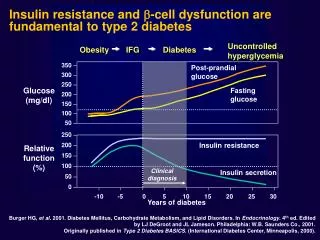
Up to 92% of people with Type 2 diabetes demonstrate insulin resistance Insulin resistance and beta-cell dysfunction can precede diagnosis of Type 2 diabetes by up to 12 years Insulin resistance can be identified by these markers: 1) Hyperglycemia 2) Dyslipidemia- high triglyceride, low HDL 3) Central obesity 4) Hypertension- greater than 130/80 Other notes…..
Abdominal fat continually releases triglycerides into the branch of the bloodstream that feeds the liver This increases the body’s need for insulin release Demand for more insulin causes the pancreas to work harder to produce elevated insulin levels High levels of insulin in blood down-regulate the affinity for insulin that insulin receptors all over the body have naturally-”tolerance” causes > IR FAT, TRIGLYCERIDES, AND INSULIN
INSULIN RESISTANCE The vicious cycle of insulin resistance Overeating Beta cell burnout Insulin Resistance Truncal obesity Excessive insulin production by reduced number of beta cells High blood sugar Craving carbohydrates Hunger
The Culprit? FAT? • And we aren’t talking about dietary fat • Triglycerides are in circulation at some level in the bloodstream at all times • High triglyceride levels are not so much the result of intake of dietary fat as they are of excessive carbohydrate consumption and existing body fat • Visceral fat-concentrated around middle of the body, surrounding the intestine
The importance of PPARy--Peroxisome Proliferator Activated Receptors are found in or on cells in muscle, fat, and liver tissue and are involved in energy metabolism PPARs regulate the action of insulin Activation of PPARy results in decreased insulin resistance which in turn helps glucose enter the cells or……..PC-1…... Or is the Culprit…?Mutations & genetic error?
PC-what? • Researchers have identified a protein called PC-1 that shuts down the insulin receptor, which creates insulin resistance • This protein is prevalent in most people with Type 2 diabetes compared to people without diabetes. Too much of the inhibitor protein is made in some people and the insulin receptor cannot do its job
How does it affect the chain? • PC-1 “desensitizes” insulin receptors. The overproduction of PC-1 is a genetically determined trait • The high levels of PC-1 protein lead to insulin resistance • A series of defects limiting function exist • FYI-Researchers are also now looking for an obesity gene
TREATMENT?--LOSE fat or ADD medicine or both • Weight reduction can reduce insulin resistance, and reduce the need for medication. Eat less! • Hypocaloric diet • Exercise • Biguanide---Metformin • Thiazolidinediones---Pioglitazone/Rosiglitazone
Biguanides--Glucophage or Glucophage XR Most widely prescribed Don’t cause hypoglycemia Does not promote weight gain Positive effect on blood lipid levels which can reduce insulin resistance Suppress liver glucose Enhances sensitivity of peripheral and hepatic tissues to insulin Thiazolidinediones--Actos (pioglitazone) or Avandia (rosiglitazone) Insulin sensitizers target insulin receptors in muscle and fat cells to increase insulin sensitivity in the body Lowers glucose-reduce hyperinsulinemia Can be effective in lowering TG levels & raising HDL’s Activates PPAR receptors to control glucose transport Biguanides vs TZD’s
In Conclusion…..IR • Upper body subcutaneous fat-obesity • Genetics-inheritance gene mutation PPAR • Protein PC-1 insulin receptor inhibitor • Combination of? • Prevention? What can an individual at risk do? Decrease upper body obesity or introduce a form of therapy than can correct the abnormal adipose tissue FFA release that may improve the metabolic abnormalities seen in upper body obesity even if weight loss is not successful
Resources • 1) Haffner SM, D’Agostino R Jr, Mykkaren L,et al. Insulin sensitivity in subjects with Type 2 diabetes: relationship to cardiovascular risk factors: the Insulin Resistance Atherosclerosis Study. Diabetes Care. 1999; 22:562-568 • 2) Harris MI, Klein R, Welborn TA, Knuiman MW. Onset of NIDDM occurs at least 4-7 years before clinical diagnosis. Diabetes Care. 1992;15:815-819 • 3) UK Prospective Diabetes Study 16: overview of 6 years therapy of type 2 diabetes: a progressive disease. Diabetes. 1995; 44:1249-1258. • 4) Marx N, Bourcier T, Sukhova GK, Libby P, Plutzky J. PPARy activation in human endothelial cells increases plasminogen activator inhibitor Type 1 expression: PPARy as a potential mediator in vascular disease. Arterioscler Thromb Vasc Biol. 1999; 19:546-551 • 5) Lovisach M, Rehman N, Carter L, et al. Distribution of peroxisome proliferator-activated receptors (PPARs) in human skeletal muscle and adipose tissue: relation to insulin action. Diabetologia. 2000; 43:304-311 • 6) Touchette P, Sherrye L, American Diabetes Association Complete Guide to Diabetes. 1999: 1:25 • 7) Bernstein R.K., Dr. Bernstein’s Diabetes Solution. 2000 • 8) Beaser R.S., Joan V.C. Hill J.V.C, The Joslin Guide to Diabetes. 2004 • 9) Saudek C.D., Rubin R.R., The Johns Hopkins Guide to Diabetes. 2001 • 10) Ford-Martin P., Ian Blumer. The Everything Diabetes Book. 2004;3:22,166-168