Download
1 / 19
200 likes | 352 Vues
Chapter 4. Developmental origins of insulin resistance and type 2 diabetes. Wen-Ying, Chen 2006, 10, 19. Preface. Epidemiological studies. type 2 diabetes Birthweight hypertension metabolic syndrome. Genetic Effects???. Environment???. Introduction.

E N D
Chapter 4 Developmental origins of insulin resistance and type 2 diabetes Wen-Ying, Chen 2006, 10, 19
Preface Epidemiological studies type 2 diabetes Birthweight hypertension metabolic syndrome Genetic Effects??? Environment???
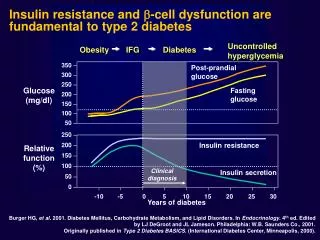
Introduction Type 2 diabetes (Hales et al., 1991) Insulin resistance (Phillips et al., 1994) Hypertension (Barker & Osmond, 1988) Low birthweight Number and secretory function of β-cells Growth of kidneys & number of nephrons
Thrifty phenotype hypothesis (Heles & Barker, 1992) Other maternal or placental abnormalities Maternal malnutrition Foetal malnutrition and low birthweight Obesity/age Other organ Decreased Insulin Abnormal Decreased Malfunction beta-cell mass resistance vascular nephron e.G liver development number Dyslipidaemia Type 2 diabetes Hypertension Metabolic syndrome
Foetal insulin hypothesis (Hattersley & Tooke, 1992) Genes influencing insulin resistance Reduced insulin-related growth Direct effect Reduced foetal growth and low birthweight Insulin resistance Susceptibility to type 2 diabetes and the Metabolic syndrome
Human studies • Twins: any differences in birthweight must be related to the foetal environment. Provide strong evidence for the importance of a non-genetic intrauterine factor in the development of type 2 diabetes in later life. • Dutch Hunger Winter: 400 to 800 kcal per day The last trimester of pregnancy is a critical time window in terms of growth.
Animal studies • Maternal protein restriction • Maternal calorie restriction • Maternal anaemia • Maternal high-fat feeding • Intrauterine artery ligation • Foetal exposure to glucocorticoids
Hormonal insults(Foetal exposure to glucocorticoids) 1.Prenatal exposure to glucocorticoidtreatment----foetal growth and birthweight retardation (Reinish et al.,1978) 2. steptozotocin a. mild maternal diabetes-----increased birthweight and beta-cell hyerplasia b. severe maternal diabetes----reduced birthweight and beta-cell mass
Surgical intervention(Intrauterine artery ligation) 1. In humans impairment in utero-placental perfusion-----intrauterine growth retardation (Bernstein and Gabbe, 1996) 2. In rats bilateral uterine artery ligation in late gestation---- glucose intolerance, insulin resistance, β-cell mass reduction and elevated glucose levels by 6 months (Simmons, Templetion and Gertz, 2001)
Nutritional models of early growth restriction • Litter size manipulation • Maternal calorie restriction • Maternal high-fat feeding • Maternal iron restriction • Low-protein model
Litter size manipulation Litter size ﹢ nutrition Litter size NPY in brain slices (appetite-controlling neuropeptides) Appetite (Winick & Noble, 1996) Obesity, hypertension and an increased susceptibility to sub-diabetogenic streptozotocin doses in adulthood (Davidowa, Li & Plagemann, 2003)
Maternal calorie restriction • Maternal diet (30% of the control) striking growth restriction, increased systolic blood pressures, increased fasting plasma insulin levels and hyperphagia • Maternal diet (50% of the control)---during the last week of pregnancy and lactation age-dependent loss of glucose tolerance placental 11β-hydroxysteroid dehydrogenase type 2 -------foetal glucocorticoid exposure
Maternal high-fat feeding High-fat feeding in pregnancy or lactation hypertension, hyperinsulinaemia and increased adiposity (Khan et al., 2005) 1.In humans High levels of dietary fat intake during gestation ---- increase the incidence of cardiovascular risk factors in children (Newman et al., 1986) 2.In rat Mothers fed high levels of saturated dietary fats ---- foetal insulin resistance (Guo and Jen, 1995), abnormal cholesterol metabolism (Brown et al., 1990) and go on to develop hypertension in adulthood (Langley-Evans, 1996)
Maternal iron restriction Offspring Maternal Hypertension 1.SBP below control in 20 day age but above control in 40 day age (Crowe et al., 1995) 2.Heart weight are increased in 20 day age--- altered cardiovascular development (Crowe et al., 1995) 3.No changes in glucose tolerance or insulin resistance at 16 months (Lewis et al., 2002) Dietary iron restriction • Hepatic lipid metabolism (Zhang et al., 2005) • 27% in cholesterol but 29% in triglyceride in liver • 2. Hepatic mRNA levels of cholesterol 7α-hydroxylase (CYP7α) were 50% and liver X receptor-α (LXRα) 34%
Low-protein model I Cross-fostered at birth to control dams 8% protein diet (control: 20%) 15% birhtweight reduction 30 % reduction in longevity (renal failure) Rapid postnatal catch-up growth during lactation Low-protein rat model displays organ-selective growth.
Low-protein model II • Isolated tissue soleus muscle and adipocytes (15-month-old low-protein offspring)-----resistant to the action of insulin and to stimulate glucose uptake. Insulin receptor expression was similar to that of controls. This suggests that the molecular basis of the insulin resistance lies downstream of the insulin receptor. a. muscle: PKCζexpression reduction b. adipocytes: p110β catalytic subunit of PI3-kinase
Low-protein model III Specific nutrients are important in preventing the detrimental effects of intrauterine growth retardation. Increased glycine ----- hypertension Maternal Low – protein diet Increased urea ---- Body weights of offspring are not reduced Supplement taurine --- rescue some of the effects on the foetus
Low-protein model IV Low-protein model in mice ---- different genetic background In leptin-deficient mice 1. leptin treatment in adulthood is unable to reverse the neuro-anatomical defect. 2. leptin treatment in the perinatal period completely restored the density of innervation to that observed in wild-type mice.
Conclusions Type 2 diabetes Hypertension Metabolic syndrome Some molecules Early environment