HPI
HPI. 63-year-old gentleman who initially presented with a five-week history of headaches behind the right eye, with associated “dizziness.” Two months prior to this, he had a syncopal episode. What questions do you want to ask your patient?. HPI.


HPI
E N D
Presentation Transcript
HPI • 63-year-old gentleman who initially presented with a five-week history of headaches behind the right eye, with associated “dizziness.” Two months prior to this, he had a syncopalepisode. • What questions do you want to ask your patient?
HPI • On further questioning, the patient’s wife notes that the patient needed help while getting dressed. He has been dragging his left leg, and he has experienced weakness of the left hand. • The patient also reports nausea & vomiting, especially upon waking in the morning. • He denies numbness or sensory loss.
Medical History • Past Medical Hx: Significant for hypothyroidism, HTN and hyperlipidemia. • Past Surgical History- None • Family History: Father died of MI • Social Hx: Non-smoker, Married with one child. Pt is an English professor. • Medication- • Atorvastatin 20mg BID • Levothyroxine 0.025mcg Daily • Hydrochlorothiazide 25mg Daily • Allergies: None • What is your differential diagnosis?
Differential diagnosis of a brain mass • CVA • Risk factors? • Localize the lesion! • Complex migraine • Seizure + Todd’s paralysis • Primary CNS neoplasm • Glioma • Meningioma • Primary CNS lymphoma • Metastatic Brain tumors • Hemorrhage • Epidural • Subdural (acute v chronic) • Intraparenchymal • Vascular disease/AVM • Infections • Abscess • Granuloma What would you like to do next?
Physical Exam Vital Signs: Temp 99.8F, BP 137/89, HR 75, RR 16 General: Pt had flat affect, his verbal responses were slow, and he was alert and oriented and in no distress. • He was afebrile and his vital signs were stable. • Neurological examination: • Motor examination revealed diminished strength in his left upper and lower extremeties as compared to the right • MSRs 2+ and equal bilaterally in the upper extremeties; 3+ left patellar/achilles ; 2+ right patellar/achilles. • Babinski sign present on the left. • Cranial nerve examination revealed R pupil slightly larger than the L. • Visual field testing revealed a defect in the upper left quadrant in both eyes. • What tests would you order?
Tests/Procedures • WBC 4000, Hemoglobin 13 (anemic if less than 12.5), Hematocrit 37 • BMP (basal metabolic panel): normal • CT scan with and without contrast revealed a large, irregularly enhancing mass in the right temporal lobe that was associated with marked edema and mass effect, with mild uncal herniation and left shift suggestive of a brain tumor. • MRI to further characterize the lesion
Resolution • Neurosurgery was consulted and the patient taken to surgery for a right temporal lobe lobectomy. • The final pathology was consistent with Glioblastomamultiforme (GBM).
GlioblastomaMultiforme- • Glioblastoma is a type of glioma/astrocytictumor. GBM represents a grade IV astrocytoma. • What are the histological hallmarks of grade IV?? • PrimaryGBM accounts for the vast majority of cases (60%) in adultsolder than 50 years. These tumors manifest de novo (ie, without clinical or histopathologic evidence of a preexisting, less-malignant precursor lesion), presenting after a short clinical history, usually less than 3 months. • Secondary GBM (40%) typically develop in younger patients (< 45 y) through malignant progression from a low-grade astrocytoma (WHO grade II) or anaplastic astrocytoma (WHO grade III).
Clinical presentation • Brain tumors can produce symptoms and signs by local brain invasion, compression of adjacent structures, and increased intracranial pressure (ICP). • How can you quickly lower ICP?? • Headache, a common manifestation of brain tumors is the worst symptom in about 50% of patients. It’s suggestive features include nausea and vomiting (~40%), change in prior headache pattern, and an focal neurologic deficits.
Histological characteristics • Macroscopically, GBMs are poorly delineated, with peripheral grayish tumor cells, central yellowish necrosisfrom myelin breakdown, and multiple areas of old and recent hemorrhages. • Microscopic , great cellularity with pleomorphism of cells and nuclearatypia; identifiable astrocytes with fibrils in combination with primitive forms in many cases; tumor giant cells and cells in mitosis; hyperplasia of endothelial cellsof small vessels; and necrosis, hemorrhage, and thrombosis of vessels
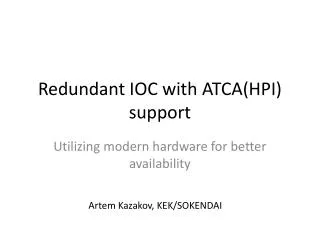
Histology specimen of a GBM with primitive neuroepithelial tumor (PNET) component mimicking a carcinoma metastasis. The tumor cells shown here had a high proliferative activity and were immunoreactive for Synaptophysin • Pallasidingis common.
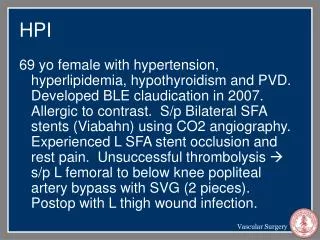
Area of Necrosis This glioblastomamultiforme (GBM) demonstrates marked cellularity with marked hyperchromatism and pleomorphism. Note the prominent vascularity as well as the area of necrosis at the left with neoplastic cells palisading around it.
MRI (Magnetic resonance imaging — Gadolinium-enhanced magnetic resonance imaging (MRI) is usually the only test needed to suggest a brain tumor. MRI may also provide information that indicates the specific tumor type. • Malignant gliomas are typically hypointense on T1-weighted images, and enhance heterogeneously following contrast infusion. Enhancing tumor can be distinguished from the surrounding hypointense signal of edema on T1-weighted sequences. • In eloquent areas of the brain, imaging after activation of sensory and motor areas by appropriate stimuli may permit separation of tumor from normal brain preoperatively
Imaging appearance is usually that of a nonhomogeneous mass, often with a center that is hypointense in comparison to adjacent brain and demonstrating an irregular thick or thin ring of enhancement, surrounded by edema. Part of one lateral ventricle is often distorted, and both lateral and third ventricles may be displaced.
Treatment • Mainstay of therapy is surgical exploration or biopsy followed by radiation and adjuvant chemotherapy • Initially, patients with GBM were given the nitrosurea, carmastuine as adjuvant alongside radiation after some studies showed small survival benefits. • Recently, temozlomide, an oral alkylating agent has become popular chemotherpeutic drug against GBMs. Its anti-tumor activity has been attributed to It’s ability to deplete O-methylguanine DNA methyltransferase (MGMT), a DNA repair enzyme. The concurrent administration of temozlomide and radiation therapy has shown significant increase in survival rates of patients with GBM. • Temozlomide has some significant drug toxicity, which caused some trials to be discontinued. Some of the sideeffects of temozlomide are leukopenia, gastrointestinal symptoms, alopecia, fatigue, and many others. • For a brief period, corticosteroids, usually dexamethasone in doses of 4 to 10 mg q6–12h, are helpful if there are symptoms of mass effect, such as headache or drowsiness; local signs and surrounding edema tend to improve as well. Antiepileptic medications (AEDs) are not required unless there have been seizures. • Variables predicting longer survival in several studies include extent of resection (gross total versus subtotal), younger age (<50 years), normal mental status, and smaller tumor volume.