Download
1 / 35
350 likes | 781 Vues
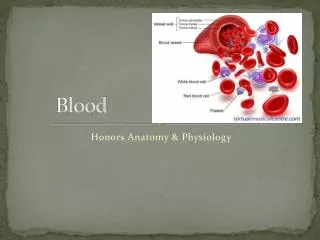
Blood transfution. Blood Transfusion. Blood Transfusion. History Type of Transfusion Indication Transfusion Reactions Autologous transfusion Component Transfusion. History and Significance. First blood transfusion. Lower (1665). First human blood transfusion. Philip (1825).

E N D
Blood Transfusion • History • Type of Transfusion • Indication • Transfusion Reactions • Autologous transfusion • Component Transfusion
First blood transfusion Lower (1665)
First human blood transfusion Philip (1825)
Discovery of ABO type Landsteiner(1900)
World war I How to store blood longer?
World war II Is there any suitable Blood Substitutes
Blood Transfusion Successful blood transfusion is relatively recent • Crossmatching • Anticoagulation • Plastic storage container
Blood Transfusion Type of Transfusion: • Whole Blood; • Blood Component; RBC PLT FFP Leukocyte concentrate • Plasma Substitutes; Use of whole blood is considered to be a waste of resources
Red Blood Cells • Symptomatic anemia (providing oxygen-carrying capacity) • Transfusion trigger (HCT<30% ; HB<10g/dl) • 1 Unit increases 3% HCT or 1g/dl • Shelf life =42 d (1-6 ℃)
Platelets • Thrombocytopenia (< 50,000) • Platelet dysfunction • Each unit increase 5,000 PLTs after 1 H
Granulocytes • Profoundly granulocytopenia (<500) • Serious infection not responsive to antibiotic therapy
Fresh Frozen Plasma (FFP) • Coagulation factor deficiencies • 1 ml increases 1% clotting factors • Being used as soon as possible • Albumin, hetastarch, crystalliods are equally effective volume expander but safer than FFP • After use of 5 U of RBCs, matching 2 U of FFP
--Volume Expander Plasma Substitutes Dextran • Most widely used • Low/Middle M.W. (40,000-70,000) • Massive transfusion could impair coagulation • Occasional ALLERGIC reaction Hydroxyethyl Starch Formulation (HES) • More stable • Containing essential electrolytes • No allergic reaction
Blood Transfusion Indication: • Acute massive blood loss; • Anaemia and hypoalbuminemia; • Overwhelming Infection; • Dysfunction of Coagulation;
Blood Transfusion Technique of Transfusion: • Approach Route: Peripheral Vein, Center Vein • Filtration before Transfusion: • Velocity of Transfusion: 5-10ml/min
Blood Transfusion Attention: • Double Check: Name, Type and Crossmatch • Storage Time: Citrate Phoshate Detrose Acidic Citrate Detrose 21D, 35D • Pre-heat: • No any other Medication: • Observation during / after Transfusion:
Transfusion Reactions Febrile Reactions : Incidence:2% Chills, Fever 39-40.C Headache, Sweatiness Nausea, Vomiting, Flushing 15min-1hr
Transfusion Reactions Febrile Reactions : • Immuno-reaction : • Endo-toxins: • Contamination or Hemolysis: Treatment: • Analyze possible reasons: • Stop Transfusion : • General Support:
Transfusion Reactions Anaphylactic reactions: Urticaria Abdominal cramps Dyspnea Vomiting Diarrhea
Anaphylactic reactions: Reason: • Immuno-reaction: IgE • Hereditary Immunoglobulin: IgA Treatment: • Administer antihistamines • Administer epinephrine, diphenhydramine, and corticosteroids: • Support airway and circulation as necessary:
Transfusion Reactions Hemolytic transfusion reactions Burning at the intravenous (IV) line site Fever, Chills, Dyspnea Shock Cardiovascular Collapse Hemoglobinuria, Hemoglobinemia Renal Failure DIC
Hemolytic Transfusion Reactions Reasons: • ABO incompatibility • Rh Incompatibility • Non-immune Hemolysis • Immune Hemolysis
Hemolytic Transfusion Reactions Treatment: • Stop Transfusion as soon as reaction is suspected • Check the name, type and crossmatch • Urine Exam • Renal Protection (Aggressive Fluid Resuscitation, Furosemide) • DIC Monitor
Hemolytic Transfusion Reactions Prevention: • Double Check name,type and crossmatch • Operate carefully and routinely • Temperature Monitor
Transfusion Reactions Massive transfusion complications: Volume Overload Congestive Heart Failure Tachycardia Tachypnea Cyanopathy
Massive Transfusion Complications: Reasons: • Volume Overload • Heart Functional Failure • Lung Functional Failure Treatment: • Stop Transfusion • Heart Functional Support • Diuresis (Furosemide)
Transfusion Reactions Contamination: Fever Shock DIC Reasons: Bacterial Contamination
Contamination: Treatment: • Stop Transfusion • Bacterial Exam and Culture • Antibiotics Prevention: • Double Check • Operate carefully
Transfusion Reactions Acquired diseases : • Hepatitis B, Hepatitis C • HIV • Cytomegalovirus (CMV) • Syphilis • Malaria
Autotransfusion: • No risk of infectious disease transmission • No transfusion reactions • No compatibility testing • Reduced demand on blood bank stores • An immediate source of autologous blood
Component Transfusion: Blood Cell: • Red Blood Cells Packed RBC • White Blood Cells • Pooled Platelets
Component Transfusion: • Saving blood source • Less likely carrier of transmitted diseases • Shortage of quality blood • Greater shelf life than whole blood • Helping to make blood safer by filtration • Infusing regardless of ABO type in some blood products giving only essential/desired blood component