Download
1 / 24
240 likes | 315 Vues
Learn how communication failures can lead to patient harmful events, recognize risks, and advocate for system improvements. Understand the impact of faulty systems vs. personal approaches in healthcare errors and the importance of a systems approach.

E N D
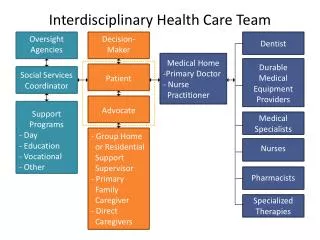
Unit 3 Health-Care Team Communication Group Processes and Patient-Safe Communication Among Team Members
Chapter 12 Patient Safety Communication Risk Factors in Nursing Work Systems
Communication Failures Result in Patient Harmful Events • Nurses must: • Learn how communication failures happen • Recognize risks for communication failure in the work environment • Use patient-safe communication strategies specific to working as a member of the health-care team • Advocate for health-care system improvements to keep patients safe
Communication is crucial to prevent harmful events in the nurses professional role • Patient Monitoring • Ongoing assessments and evaluation of patient health state to maintain situational awareness, with the need for communication with team members for clinical decision making • Health-care providers form a mental model of the patient’s clinical situation and make clinical decisions based on the nurse’s shared essential information • Coordination of Care • Communicate to coordinate patient care and services from multiple members of the health-care team • Maintaining Continuity of Care During Transitions • Communicate patient status and plan of care across care continuums
The Institute of Medicine Report • 44,000 –98,000 deaths occur as a result of medical errors • One death every 5 – 10 minutes • Nearly 70% of these deaths related to communication failures • Cost associated with medical errors is $8–$29 billion annually • Since 2000, when the report was published, little progress has been made to reduce the numbers of harmful events
Reducing Patient Care Errors:Systems vs Personal Approach • Systems approach • Recognizes people are fallible and make mistakes • Does not hold professionals accountable for system failures • Does not tolerate gross misconduct of individual • Personal approach • Blames, names, shames, and retrains individuals committing errors • “Bad” people make errors Health-care organizations are slow in adopting a systems approach
Failed communication is the reason for nearly 70% of Sentinel Events
Why Do Errors Occur? System Approach • Faulty health-care systems • Faulty processes within health-care systems • Poor working conditions • Lead individuals to make mistakes • Not the result of individual recklessness of health-care providers • Health-care system is the problem and needs to be made safer
Health-care errors are symptoms of an unsafe system • Conditions within the nursing work system affect human performance leading to patient-care errors • More acutely ill patients • Shorter hospital stays • Frequent patient turnover • Extended hours and overtime • Stressful work environment • Interruption-driven environment • High nursing workloads
Health-care team members will improve safety by taking a systems approach: • Understanding system design and the impact on safety • Risk awareness through anticipating and recognizing safety problems • Correcting safety problems to prevent harm to patients
Systems approach requires knowledge of human factors science • Study of the “fit” between people, • The things they do • The objects they use • The environments in which they work. • If a good “fit” is achieved, it reduces stress on people
Human Abilities and Limitations Affecting Performance • Human strengths • Creativity • Adaptability • Flexibility • Good at finding explanations and meanings from ambiguous evidence and developing a work-around or “quick fix” when things do not work as well as desired • Human weakness: Humans make errors • 90% of all organizational accidents result from human error • Human error is the failure of a planned action to achieve its intended goal • Humans are fallible: • Cannot maintain continual alertness • Inability to attend to several things at once • Have habits of thought and action • Lack precision in mental functioning
Normal Cognition Theory: How People Think During Performance of Activities • Automatic mode—often repeated, routine tasks • Conscious mode—conscious critical thinking in new situations • Mixed mode—during trained-for situations
Types of Human Errors • Errors of Execution • The plan is adequate but does not proceed as intended • Skill-based error—attention or memory failures • Errors of Decision Making • The wrong plan is used to achieve an aim • Rule-based error— apply the wrong rule to a patient situation • Knowledge-based error—lack of knowledge, lack of information or misinterpretation • Violations • Deliberate deviations from standard practices, policies, and procedures • People purposely break rules with poor operating procedures, inadequate work environments, low morale, time pressures, and inadequate tools and equipment causing frustration
The Nursing Work System • System defined: Interdependent components that interact to achieve a common goal • Nursing work system: Interdependent components of the health-care system • Levels of hierarchy: • Higher levels provide context for lower levels (context = policies, procedures, norms, technologies, physical environment, people) • Changes at one level affect all other levels, affecting individuals, groups, or the organization • Higher-level decisions can exert influence that unexpectedly contributes to work conditions that lead to human error
The Nursing Work System • Performance inputs—guide the nursing work system • Process—changing inputs into outputs through human behavioral performance • Performance outputs—outcome of the inputs and process • System inputs influence nurses’ ability to perform work activities that will affect patient outcomes • A well-functioning system can facilitate performance • A poorly functioning system creates conditions that lead to human errors
How System Factors Create Hazardous Conditions • Accident Causation Theory • When system components across levels function well together, they collectively serve as barriers to prevent harmful events • E.g., adequate staffing and appropriate workloads • When weaknesses in the system interact in a way to breach barriers, harmful events occur • E.g., inadequate staffing and heavy workloads
System Defenses as “Swiss Cheese” • System defenses have many holes • These holes continually open, close, and shift • Harmful events happen when the holes in many successive system levels momentarily line up and propel a trajectory of error leading to a harmful event
System defense holes occur for two reasons • Active failures—unsafe acts that are human errors • Attention slips • Memory lapses • Honest mistakes • Intentional violations • Latent conditions—flaws within the work system due to decisions made by managers and top-level administrators • Poorly designed facilities • Training gaps • Staff shortages • Heavy workload • Inadequate communication processes • Faulty policies and procedures
Mental Antecedents to Active Failures and Unsafe Acts • What goes on in the mind of the health-care provider prior to an active failure with an unsafe act • Distraction, momentary inattention, forgetting, losing the picture, preoccupation, fixation • Environment can be hectic, demanding, time-pressured, and inadequately staffed
Systems Approach: Focus on Latent Conditions • Determine underlying cause for active failures • Focus on changing conditions in the system that contribute to human error • Nurses who have the greatest contact with patients are positioned to detect and correct health-care errors before they reach the patient • Nurses must speak assertively about latent conditions • Nurses must develop situational awareness of the high-risk environments in which they work
Nurses must identify and correct latent conditions in the nursing work system • Unworkable procedures • Unrealistic policies • Design deficiencies in nursing work areas • Error-provoking conditions leading to unsafe acts (overburden human limitations) • Time pressures • Heavy workload • Understaffing • High cognitive demands • Interruptions • Long hours • Inadequate training • Unavailable essential information • Inadequate communication processes