Download
1 / 40
410 likes | 632 Vues
ICH Public Meeting January 21, 2003 5630 Fishers Lane, Room 1066. FDA PERSPECTIVE IMPLEMENTATION STATUS OF THE CTD. Justina A. Molzon, M.S. Pharm., J.D. Associate Director for International Programs Center for Drug Evaluation and Research/USFDA CDER ICH Steering Committee Representative.

E N D
ICH Public Meeting January 21, 2003 5630 Fishers Lane, Room 1066 FDA PERSPECTIVE IMPLEMENTATION STATUS OF THE CTD Justina A. Molzon, M.S. Pharm., J.D. Associate Director for International Programs Center for Drug Evaluation and Research/USFDA CDER ICH Steering Committee Representative
Practical Issues of Implementation • Finalized CTD presented at ICH-5 • 9-11 November 2000,San Diego • Three separate groups working in isolation to get the documents done on time • Had to edit for consistency • Numbering systems • Style • Format
Reality of Implementation • Once regulators started preparing documents for publication, realized how complicated they are • Faced with the enormous task of making them consistent • Regulators have different systems • No matter how closely we work together will still have some minor inconsistencies
I C HINTERNATIONALCONFERENCE ONHARMONIS/ZATIONof Technical Requirements for the Registration of Pharmaceuticals for Human Use
Reality of Implementation • Complications and minor inconsistencies don’t detract from the enormous work that has been done • We want the CTD to be the best it can be • Must work hard to do away with ambiguities and inconsistencies • An evolving process
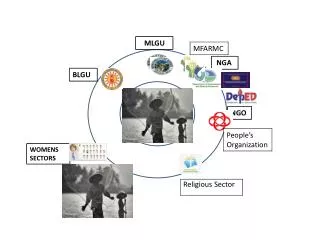
Module 2 NonclinicalOverview ClinicalOverview NonclinicalSummary ClinicalSummary NonclinicalStudy Reports ClinicalStudy Reports Quality Module 3 Module 4 Module 5 The CTD Triangle NOT Part of the CTD RegionalAdminInformation Module 1 The CTD QualityOverallSummary
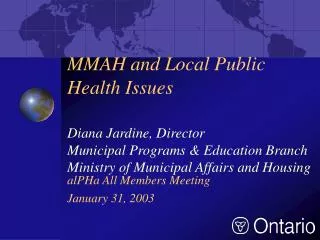
May 2001 Steering Committee 1.0 Regional Administrative Information 1.1 ToC of Module 1 or overall ToC, including Module 1 2.1 ToC of the CTD (Mod 2,3,4,5) 2.2 Introduction 2.3 Quality Overall Summary 2.4 Nonclinical Overview 2.5 Clinical Overview 2.6 Nonclinical Summary 2.7 Clinical Summary Numbering System Module 1 1.0 2.1 Module 2 2.2 2.5 2.4 2.3 2.6 2.7 Module 3 Module 4 Module 5 Clinical Study Reports 5.0 Nonclinical Study Reports 4.0 Quality 3.0 Source: ICH Implementation Coordination Group
Practical Issues of Implementation • Need to work with other regions • Need experience with documents • Meetings a big help in pointing out areas which can be improved • Submissions will help industry and regulators gain familiarity with the new format • Reason voluntary submission phase extended from 2002 to July 2003
An Overview of the CTD • The CTD is not a “Global Dossier”! • Content different for US, EU and Japan based on individual regulations • Some regulations never covered in ICH • It is an agreed upon common format for the “modular” presentation of summaries, reports and data • Incorporates relevant ICH guidelines as building blocks and puts them in the same order for submission to ICH regions
CTD General Questions and Answers • Question #1 • Will a dossier using the CTD format (Modules 2 to 5) be identical for all regions? • Answer #1 • Not necessarily
Answer • The CTD provides a common format for the submission of information to regulatory authorities in the three ICH regions. • However, the CTD does not address the content of submissions. • Regional requirements • Applicants preferences
DRAFT Guidance Publication • Submitting Marketing Applications According to the ICH/CTD Format: General Considerations (DRAFT) • Posted September 5, 2001 • Comment period until November 5, 2001 • 12 sets of comments submitted • Comments always welcome • In process of reopening docket • Will incorporate comments from SC/EWG and outreach meetings into final draft this spring
CTDGeneral Considerations Guidance • What we expect to be submitted • Description of Module 1 • Administrative/Prescribing Information • Physical description of submission • CTD requirements addressed • Obsolete guidances listed • Logistics of submission described • Timeframe for submission
Electronic Submission • The General Considerations Guidance describes the organization of an application provided entirely in paper • Also describes how to adapt the CTD to our current process for electronic submissions • May provide documents electronically (in PDF format) instead of on paper
CTD Guidance Publication • M4: Common Technical Document for the Registration of Pharmaceuticals for Human Use • Posted October 15, 2001 • Kept in review discipline format for ease of printing and navigating • Safety appendices split off because of size • Posted in WORD so companies can populate tables with data
CTD Guidance Publication • M4: Organization of the CTD • M4: The CTD -- Quality • M4: The CTD -- Efficacy • M4: The CTD -- Safety • M4: The CTD -- Safety Appendices • POSTED ON CDER WEB http://www.fda.gov/cder/guidance/index.htm
CDER CTD Submissions • 11 submissions in CTD Format • 7 different Review Divisions • All 5 Offices (ODE 1-->5) • Several CTDs for new dosage forms • Several rolling submissions • Hybrids (Safety or Quality Modules) • Paper and electronic submissions
Office of Drug Evaluation I Division of Oncology Drug Products • Received: August 1, 2001 • CTD: Pharmtox section submitted electronically • Fast track rolling submission
Office of Drug Evaluation IV Division of Special Pathogen and Immunologic Drug Products • Received: October 22, 2001 • CTD: Uses CTD table of contents • Structure is not as recommended but close
Office of Drug Evaluation VDivision of Anti-Inflammatory Analgesic, and Ophthalmologic Drug Products • Received: Dec 27, 2001 • Different dosage form • CTD: Pharmtox, presubmission in CTD format • The application consists of a paper copy and electronic copy
Office of Drug Evaluation III Division of Reproductive and Urologic Drug Products • Received: December 31, 2001 • CTD: Only the chemistry section is in the CTD format • Submitted on paper • Electronic sections not in CTD format.
CDER CTD Submissions • No refuse to files • Not perfect submissions but could be reviewed • Flexible during voluntary submission phase • Through July 2003 • July 2003--Mandatory in EU, Japan, highly recommended in US. • Further training based on practical experience • Encouraged to submit in CTD format • Hybrid submissions acceptable
CTD Pre-submissionExperience • Submission should exactly match CTD • 3.2.S.1.2 -- The structural formula, including relative and absolute stereochemistry, the molecular formula and the relative molecular mass should be provided. • Provide all information under CTD ICH negotiated headings and numbers • Do not create new headings or numbers
CTD Pre-submissionExperience • DO NOT modifiy CTD TOC numbering system by adding additional levels • 3.2.S.1.2 Structure • 3.2.S.1.2.1 Molecular Formula • 3.2.S.1.2.2 Molecular Weight • Provide all information under CTD designated headings • May use subheaders or bullets
CTD General Questions and Answers • Question #5 Sub-Heading Numbering or Numbering within Sections • How should sub-numbering within a document be organized? Some documents can be up to 50 pages in length with no defined CTD guideline heading and potentially no TOC entries or bookmarks
Answer • Within the document, the applicant can use section numbers at a lower level than those specified in the CTD guideline. However, there should be no other headings appearing in the overall TOC going below the numbering given in the CTD guideline
CTD Pre-submissionExperience • If you don’t have information for a section provide: • ICH CTD Number and Header • NA (not applicable) or other language • Don’t skip or delete section • Never renumber sections • See CTD Safety Q&A #2
CTD Pre-submissionExperience • CTD-Q 3.2.R -- Regional information is for unique regional information • Unique=Information that does not have a general topic designation in Module 3 • Adhere to examples Listed in 3.2.R • Even though requested information may be unique to FDA, insert information in appropriate CTD-Q topic section • DO NOT place in Regional Information
CTD IWG/EWG Meetings9-12 September 2002 • Main topic for discussion • LOCATION-LOCATION-LOCATION • Especially for CTD-Q • Comparing to FDA DRAFTDrug Product and Drug Substance Guidances for Chemistry, Manufacturing and Controls Information • Location of information in CTD will be detailed by DRAFT Guidances • See CTD-Quality Q&A’s
CTD IWG/EWG Meetings9-12 September 2002 • Revised--Organisation of the Common Technical Document for the Registration of Pharmaceuticals for Human Use • Numbering and section headers have been edited for consistency and use in the e-CTD • Granularity document provides guidance on document location and pagination • Q&A’s for each Module (S, E, Q) posted on ICH web for clarification
CTD IWG/EWG Meetings9-12 September 2002DISCLAIMER • The final ICH CTD adopted version is published on the ICH website. • At regional level a local version is published. • The wording of the core CTD may be slightly different from one region to another due to specific editing and local regulation. • It does not affect the common understanding by the six parties of the CTD published on the ICH website.
eCTD • Six months behind CTD • The eCTD will be a transport format to be moved into an agency’s review environment • Step 4 reached in Washington DC September 2002 • Biggest Payoff--eliminate controversy • A4 vs. 8 by 11 inch paper
NonclinicalOverview ClinicalOverview NonclinicalSummary ClinicalSummary NonclinicalStudy Reports ClinicalStudy Reports Quality Module 3 Module 4 Module 5 NOT Part of the CTD The CTD Triangle RegionalAdminInformation Module 1 Module 2 The CTD QualityOverallSummary
CTD Major Issue Integrated Summary of Safety Integrated Summary of Efficacy • The name”summary” has caused great confusion • Not a summary but an integrated analysis • Critical components of the safety and efficacy review and expected to be part of FDA submission.
FDA’s ISS/ISE • Clarifying what remains of the Guideline for the Format and Content of the Clinical and Statistical Sections of an Application, July 1988 • Integrated summary of safety section page 32 to 46 • Integrated summary of efficacy section page 28 to 32 • Likely to be updated as part of PDUFA-3 risk management initiative
FDA’s ISS/ISE • If what is called for in the FDA Guidances can be incorporated into the CTD, it will be a complete substitute for the analysis • If not, it will need to be submitted as a separate document • If ISS is volumes a summary • If ISE >200 pages a summary • Concerns should be raised with FDA staff prior to submission
CTDNext Steps--Training • Prior to ICH-5 CDER rolled out CTD documents with review disciplines • Met with senior project managers to provide updates • Waiting for submissions for the next phase of training • Reviewers with CTD experience will provide practical training
Impact of the CTD • The ICH CTD represents one of the most ambitious and successful international harmonization activities undertaken. • It will significantly reduce time and resources needed by industry to compile applications for global registration.
Benefits of the CTDFDA Perspective • More “reviewable” applications • Complete, well-organized submissions • More predictable format • More consistent reviews • Easier analysis across applications • Easier exchange of information • Facilitates electronic submissions • BETTER DRUGS TO PATIENTS FASTER