SURGICAL ASEPSIS & WOUND CARE
570 likes | 1.23k Vues
SURGICAL ASEPSIS & WOUND CARE. Professor Patricia Voelpel HNI 364 Fundamentals of Nursing. Introduction to Asepsis. Asepsis Is the absence of germs or pathogens. Aseptic technique: is an effort to keep the client free from hospital microorganisms. Medical asepsis : “clean technique”

SURGICAL ASEPSIS & WOUND CARE
E N D
Presentation Transcript
SURGICAL ASEPSIS & WOUND CARE Professor Patricia Voelpel HNI 364 Fundamentals of Nursing
Introduction to Asepsis • Asepsis • Is the absence of germs or pathogens. • Aseptic technique: is an effort to keep the client free from hospital microorganisms
Medical asepsis: “clean technique” Includes procedures To minimize # of microorganisms and their spread Surgical asepsis “sterile technique” Includes procedures to eliminate microorganisms and spores. Medical vs. Surgical Asepsis
Fistula and invasive lines • AV Fistula is used for a patient with renal failure. • Cordis cathether (introducer) • Which technique would a nurse use to change the dressing over the cordis?
Contaimination • Is any object that becomes unsterile or unclean. • Any object that is touched by an unsterile object is considered contaminated in a surgical aseptic procedure. It should be discarded and replaced. • Example: anything that falls on the floor, bed side tables not cleaned, a bedpan, wet gauze lying on a bedside table or bed.
The nurse’s responsibility • A nurse’s failure to be meticulous, places the client at risk for an infection that can impair recovery. • There is NO COMPROMISE to sterile technique. • Ex: washing hands, cleaning and draping a bedside table before a dressing change , inspecting packages to ensure integrity etc.
Nosocomial infections • Nosocomial infection • Iatrogenic infection • Exogenous nosocomial infection • Endogenous nosocomial infection
The cost of noscomial infection: Increased length of stay Increased disability Delayed healing Prolonged recovery Increased risk for secondary medical problems The nurse’s role Protect the patient! Use proper technique Insuring others do so also Identify breaks in technique and stop them Noscomial infections
The Rules of Surgical Asepsis • Sterile to sterile • Out of sight equals contaminated! • Do not turn back on sterile field • Nothing below the waist • Hands in front as close together as possible
The Rules continued: • Hand washing before & after each procedure • No coughing, sneezing, talking over a sterile field. If you have a cold then wear a mask. • Hold things up • Edges of a sterile field are out of bounds
The Rules continued: • Solutions: must be dated, timed and labeled. Always lip your bottle before reusing it. 24hours is the maximum parking time for any solution. When in doubt –throw it out! • Open sterile packages away from you. • All items penetrating the skin or cavity should be sterile.
The Rules continued: • No boarding house reach!! DO NOT reach across a sterile field. • Check out expiration dates and evidence of sterilization. • Protect your patients
Wounds • Defined: is a disruption of the normal anatomical structures and function that results from a pathological process beginning internally or externally to an involved organ • The classification of wounds are based on 1) status of skin integrity 2) causes of the wound 3) severity or extent of tissue injury or damage 4) cleanliness of the wound 5) descriptive qualities (color, swelling, drainage, etc.)
Status of the skin integrity • Open-break in skin or mucous membranes • Closed- wound without break in skin integrity
Causes of wounds • Intentional:wound resulting from a therapeutic procedure- Ex: incision or injection • Unintentional: wound unexpected. Usually a traumatic injury. Ex: knife wound or burn.
Severity of an injury • Superficial: involves only the epidermal layer • Penetrating: break in the epidermal surface, dermis, deeper tissue & organs • Perforating: foreign body enters and exits an internal organ
Wound classification and cleanliness • Clean: no pathogens in the wound. The closed surgical wound has not entered the GI, Resp, or uninfected GU tract, or or pharyngeal cavity. • Clean contaminated: wound made under aseptic technique condition, but involved a body cavity that normally harbors microorganisms.
Wound classification and cleanliness continued: • Contaminated: wound existing under conditions in which the presence of microorganisms are likely. Example: open, traumatic, accidental wounds or surgery with break in asepsis • Colonized: wound containing microorganisms (usually multiple). Such as in a chronic wound (vascular stasis ulcers, or pressure sores)
Descriptive classification of a wound • Laceration: tearing of tissue with regular borders • Abrasion: superficial wound involving scraping of skin’s surface • Contusion: closed wound caused by a blow to body by a blunt object characterized by swelling, discoloration, and pain.
General principles of wound healing There are 2 types of wounds: those with loss of tissue & those without loss of tissue Clean surgical incisions – wound with little or no loss of tissue heals by first intention. The skin edges approximate and the risk for infection is low. Burns, severe lacerations & ulcers have tissue loss & heal by secondary intention. Edges don’t approximate. The wound is left open until scar tissue fills the wound. The risk of infection is greater.
General principles of wound healing continued: • Third intention healingis a delayed wound closure that is deliberate attempt by the surgeon to allow effective drainage and cleansing of a clean contaminated or contaminated wound. The wound will not be closed until all evidence of edema and wound debris has been removed. As granulation tissue (scar tissue) occurs the wound will be closed by first intention process.
Healing • GI tract- scar tissue can cause ADHESIONS which may lead to pain and alteration in bowel elimination • Bone healing-1st stage is soft tissue healing. Blood clots occur between the ends of the bones. Granulation tissue then forms called procallus. 2nd stage-osteoblast enter the area and form cartilaginous tissue called callus.(similar to bone except it does not have calcium salt. Tends to be softer). 3rd stage-tissue remodels and calcium salt is laid down resulting in stronger bone.
Healing • Nerve tissue healing: • Central nerves do not heal • Peripheral nerves have shown to regenerate. • Schwann cells form a sheath around the nerve fiber which is the key to regeneration. The avg regeneration is 2mm/day. • If the connective tissue growth occurs over the path of the nerve fibers, the growth will be stopped. Hence there needs to be careful alignment of the nerve fibers at the close of a surgery to ensure healing.
Healing by Primary Intention • Inflammatory Phase: • Begins within minutes of injury and last for about 3 days • Hemostatis occurs • Migration of WBCs into the area • Epithelization begins
Healing by Primary Intention Continued • Fibrin matrix is laid down, creating a scaffold or frame work. (cellular repair) • Damaged tissue releases histamine, resulting in vasodilation of surrounding capillary and exudation of of serum. Clinical evidence of localized redness, edema, warmth and throbbing.
Healing by Primary Intention continued: • Destructive Phase: • Last 2-5 days and begins before the inflammation phase ends • Macrophage clear wound of debris and stimulate fibroblast formulation (synthesizes collagen which = strength) • Collagen is a main component of scar tissue (granulation tissue) • Fibroblast req. Vit B & C, O2, amino acids as their building blocks
Healing by Primary intention continued: • Proliferative Phase: • Begins in 3 days and last up to 24 days • Wound closes with new tissue • Degree of stress on wound determines amount of scar tissue. In general, more scar tissue will form on a mobile extremity vs. a scalp.
Healing by first intention continued: • Maturation phase: • Final phase of healing • Begins as early as 3wks or may take up to 1 year! • Collagen scar gains strength. Sometimes may be inelastic. • The scar tissue contracts, flattening and decreases the size of the wound. When palpated will feel firm. • The wound is no longer red in color and usually will be pink then flesh tone.
Healing by Secondary Intention • Large wounds with tissue loss take longer to heal, drain more fluid, fill with fragile granulation tissue. • Wounds heal from the bottom up with the granulation tissue. • Granulation tissue is form of connective tissue that has more abundant blood supply than collagen
Healing by Secondary Intention continued: • Wound contraction involves movement of dermis and epidermis on each side of the wound. Begins on the 4th day • Myofibroblast is motive force. • Wound contraction results in thinning of surrounding tissue • The size & shape of the final scar corresponds to tension lines in the damaged area. • Issues of cosmetic appearance & functionality loss due to scar tissue
Regeneration and tissue healing • If the body can not replace the tissue lost then scar tissue is formed • Scar tissue replaces the structure of the same tissue but does not replace the cellular function • Regeneration occurs with ease in the skin and mucous membranes, unless the area of injury is deep or large. • Muscles that have been severely damaged and replaced with scar tissue may be less able to contract and will be at an increased risk of strain or injury.
Factors that affect healing • Age • Nutrition and body mass index • Oxygenation of cells • Circulation • Hormones • Rest
Factors that affect healing continued: • Foreign material • Necrosis • Infection • Tissue separation-3 types
Tissue separation-Fistula • Is an abnormal passage between two organs or between an organ and outside the body. • Sometimes created intentionally by surgeon for TX reasons, may be the results of poor wound healing, trauma, radiation exposure, infection, disease state, cancer, and chronic drainage tracts.
Tissue separation -Dehiscence • When the wound fails to heal properly, the layer of skin and tissue separate. Most commonly occurs before collagen formation (3-11 days after injury). • Defined as the partial or total separation of the wound layers
Continued • At risk are the malnourished, infections, and morbid obese • May occur with exaggerated coughing, vomiting or straining. Prevented with splinting the incision!!
Tissue separation-Evisceration • Is the total separation of the wound layers. • With protrusion of the organs through an opening. • This is a true MEDICAL EMERGENCY • What actions should be taken by the nurse?????
Types of wound exudate • 1. Serosangous • Blood tinged amber fluid consist of serum • Normal for 1st 48hrs after injury • Sudden increase in amount precedes wound dehiscence in wounds closed by 1st intention
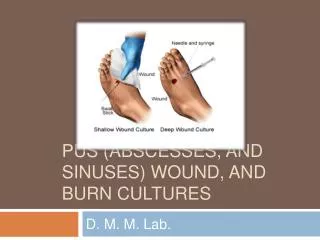
Types of wound exudate 2. Purulent • Characteristic: creamy yellow pus, greenish-blue pus causing stain on dsg w/ “fruity odor”, brownish pus w/ “fecal odor” • Significance: colonization w/ staphylococcus, pseudomonas, proteus, aerobic colliform and bacteroides (usually after Gi surgery)
Common dressing techniques for wound debridement • Wet To Dry Moistened Gauze • Wet To Damp Moistened Gauze • Continuous Wet Gauze • Topical Enzyme Preparation • Hydrophilic Beads • Moisture Retentive Dressing