Download

1 / 60
600 likes | 738 Vues
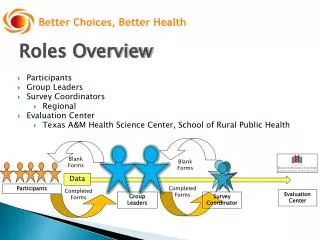
Integrated Care Management (ICM): Positioning Home Care as a Value Added Partner. Better Health Better Care Lower Cost. Learning Objectives. Provide an overview of healthcare reform and the urgency for change in our care delivery model

E N D
Integrated Care Management (ICM): Positioning Home Care as a Value Added Partner Better Health Better Care Lower Cost
Learning Objectives Provide an overview of healthcare reform and the urgency for change in our care delivery model Provide an overview of Integrated Care Management (ICM) and key best practices , competencies, and tools Review a leadership best practice to lead transformational change and clearly communicate Home Health as value added partner .
What is the Sutter Center for Integrated Care (SCIC)? • SCIC supports health care organizations, leaders and clinicians through the provision of educational programs, consultation, best practice tools, and model hardwiring of the Integrated Care Model (ICM). • SCIC team seeks to transform healthcare delivery nationwide by guiding the way for those seeking to achieve better health, better care, and lower costs for individuals and populations. • Those trained include: hospital executives, case managers, home health and hospice clinicians, care navigators/managers for hospitals and insurers, telehealth nurses, social workers, pharmacists, therapists, and physicians
Meet the Team Paula Suter, RN, BSN, MA Clinical Director Beth Hennessey, RN, MSN Executive Director Jennifer Pearce, MPA Health Literacy Program Manager
Sutter Health at a Glance • One Sutter: • Patient Experience • Operational Excellence • Market Growth • Future Innovation • 5,000+ physicians • 55,000+ employees • 24 acute care hospitals • Home Health, Home Infusion, Hospice, DME • Long-term care services • Health care research, development and dissemination program
Sutter Center for Integrated Care (CIC):Facts About Who We Serve Sutter CIC SCAH Northern California 28 Locations • 11 Home Health • 7 Hospices • 2 Infusion • 2 HME • 1 Private Duty & Geriatric Care Management 1,800 Employees 770 Volunteers 20,000 Average Daily Census Sutter Health: Transitions of Care, Complex Case Management, Advanced Illness Management, PCMH, Patient Experience, Population Health Outside SCAH/SH: 7000+ Providers (49 States and 3 Countries: US, Canada & Singapore)
Urgency for Change • STAR • CoP revisions • Value Based Payments
Star Ratings:Pay Close Attention to Patient Experience Patient Satisfaction – Did you like what I did? Versus Patient Experience – Did we do what you expected /what met your needs?
Medicare Payments Will Significantly Change: Bold Goals Are Set Alternative Payment Models ( ACOs & bundled payments) 30% by 2016 50% by 2018 2) Tied to quality or value 85% by 2016 90% by 2018
Living in Two Worlds at the Same Time is Challenging Value Based Population Reimbursement Fee for Service Urgency for change to survive and thrive in both worlds calls providers to … consistently provide exceptional high quality care for ALL patients
Evolving “World” of Payment Reform: Impacting “Transitions of Care”
Integrated Care Management (ICM): Where it started Journey Towards Excellence In Homecare & Healthcare: Improving Experience and Outcomes of Care
The Right Thing to Do:IOM Quality Chasm Report • Current healthcare systems cannot do the job • Trying harder will not work • Changing care systemswill work • Make the right thing to do the easy thing to do
The Right Thing to Do:IOM Quality Chasm Report ALL health care providers should pursue six major aims: • Safe • Effective • Patient Centered • Timely • Efficient • Equitable “ A New Health System for the 21st Century” (IOM, 2001) “Providing care that is respectful of and responsive to individual patient preferences, needs, & values & ensuring patient values guide all clinical decisions.”
Integrated Care Model (ICM):What is it? • A person-centered care delivery model • Based on Wagner’s Care Model • Integrates care transitions best practices • Integrates health literate care • All patients • Allproviders • All settings
Integrated Care Management (ICM):A Care Delivery Model for Improved Outcomes Improved outcomes leading to better health, better care and lower cost
Patients Values, Needs and Preferences Guide All Care “We think our job is to ensure health and survival. But really it is larger than that. It is to enable well-being. And well-being is about the reasons one wishes to be alive […] those reasons matter all along the way.” Atul Gawande, MD, MPH, Author of Being Mortal: Medicine and What Matters in the End
Person-Centered Care • Goal Before: • Manage signs and symptoms of HF exacerbation, low sodium diet, and fluid restrictions adhered to by ---- • Person-Centered • - Care with dignity and respect • - Value, needs and preferences drive care • - Patient as partner • Goal Now: • Able to join ROMEO (Retired Old Men Eating Out) group for lunch once a week
Person-Centered Care • Goal Before: • Safely ambulate 100 feet with or without assistive devices by time end of episode. • Person Centered • - Care with dignity and respect • - Values, needs, & preferences drive care • - Patient as partner • Goal Now: • Be able to walk on my own to the activity center in the next month.
Asking questions to understand persons preferences These are some things you can work on that will help you return to gardening. Lets go over these options together. What would you like to work on?
Power Point Template 3 Use Shared Decision Making Approach to Goal Setting Walk 15 minutes each day Starting tomorrow Walk around my house for 15 minutes after lunch daily for the next week I may feel too tired to do it “I would like to exercise” Ask my husband to encourage me Will improve my enegy level so I can work in my garden again March 2nd
Quality of Life Tools As a persons condition changes, their needs and preferences change. Shared decision making with patient and caregivers is facilitated with person-centered health literate tools.
Evidence-Based Care Step 3 • Evidence-Based • - Clinical best practices • - Patient Engagement: • Self-management support • Health literate care Step 2 Step 1 Source: Blue Shield California Foundation. (2012). Empowerment and engagement among low-income Californians: Enhancing patient-centered care.
Patient Engagement is “The Right Thing To Do” Evidence reveals that patients who are actively involved in their health and healthcare: • Achieve better clinical outcomes • Have lower healthcare costs • Are more satisfied with their care experience
How Can You Start Engaging Patients? The Cycle of Patient Engagement START HERE Source: Blue Shield California Foundation. (2012). Empowerment and engagement among low-income Californians: Enhancing patient-centered care.
This Approach is Appropriate for All Individuals Regardless of: Source: Smith, Sandra A. (2001). Patient Education and Literacy in Labus, A. & Lauber, A. (Eds.) Preventive Medicine and Patient Education. Philadelphia: WB Saunders, 266-290.
To Improve Understanding and Engagement Use a universal precautions approach to health literacy with verbal and written materials
Universal PrecautionsOral Communication Self Assessment Found in AHRQ Universal Precautions Tool Kit
Power Point Template 3 Enhancing Provider Competencies:Make “the right thing to do, the easy thing to do”
Verify UnderstandingTeach-Back Competency Check List • You get to hear in the patients own words : • their understanding • what is important • how to best “connect” new information
To Improve Understanding andEngagement Use a universal precautions approach to health literacy with verbal and written materials
Evidence: Easy-to-read is Preferred! College educated readers’response to health information written at 5th grade level: Recall of key messages Satisfaction Sources: Smith SA. Information giving: Effects on birth outcomes and patient satisfaction. Int Electronic J Health Educ 1998:;3:135-145. Online at http://www.beginningsguides.net/content/images/stories/info-giving.pdf
Health literate stoplight tool with universal precaution approach applied ClearMark Award of Distinction Center for Plain Language Washington, D.C.
Moving toward Health Literate Care:Stoplight form before • Third person • Zones drive navigation • Graphic does not support text • Font, layout, graphics not consistent with health literacy principles
Stoplight after: supports patientand family engagement • First person • Patient daily assessment drives navigation • Font, layout, graphics consistent with health literacy and plain language principles • Supports patient and caregiver engagement • Supports teach back with content ready for “chunk and check”
Universal Precautions Approach in Action: Patient Friendly Medicine List Medication and Route Frequency Reason Dose Instructions Font size increased to 14 pt
Coordinated Care • Coordinated Care • - Seamless transitions across providers, settings and time • - Meaningful and timely information exchange
Person-Centered Care “Always Event”:Starting in Hospital “I have four areas we need to focus on to help prepare you and your family for discharge, but before we start on my list can you tell me what you are the most concerned or worried about when you leave here and go home?” Then transitions of care focus areas …. 1. Medication Management Post-Discharge 2. Early Follow-up 3. Symptom Management 4. Personal Health record
Person-Centered Care “Always Event”:Starting in Hospital Feeling lonely as I live alone. Open ended questions in hospital and continued in the home • What are you most concerned about at this time? • What would you like to have happen as a result of our care? • How would you like to feel? • What is one thing that is most important to you that you want to be able to do again? Always Event
Person Centered Assesment Tool Personal assessment of health, “In general would you say your health is… poor (1) fair (2) good (3) very good (4) excellent (5) ?”
Single Item Self-Rating and One Year Event Rates Source: DeSalvo, et.al., Health Services Research, August 2005
ICM Transitions of Care:9 “Touch-Points” in First 2 Weeks Week 1 Home visits continue based on need Week 2
High Alert Medication Stoplight Tools A recent study found that four agents were responsible for 2/3 of all drug related hospitalizations: 1. Plavix 2. Coumadin 3. Insulin 4. Oral Hypoglycemics Source: Budnitz, et al. NEJM, Nov 24, 2011.
Cohesive Care Delivery Promotes Efficiency, Safety, and Access
What “key lesson” would I share with Home Health Leaders …. Source: Vocera Experience Innovation Network