Diphtheria
Diphtheria. Dr. Harivansh Chopra, MD, DCH Professor, Department of Community Medicine, LLRM Medical College, Meerut. harichop@gmail.com. Objectives. To study the epidemiology of Diphtheria. To study the complications of diphtheria, and their management.

Diphtheria
E N D
Presentation Transcript
Diphtheria Dr. Harivansh Chopra, MD, DCH Professor, Department of Community Medicine, LLRM Medical College, Meerut. harichop@gmail.com
Objectives • To study the epidemiology of Diphtheria. • To study the complications of diphtheria, and their management. • To study the treatment and prevention of Diphtheria. Dr.Harivansh Chopra
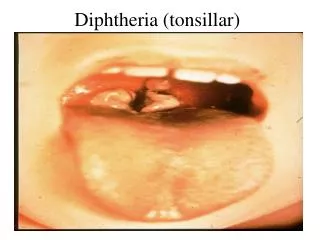
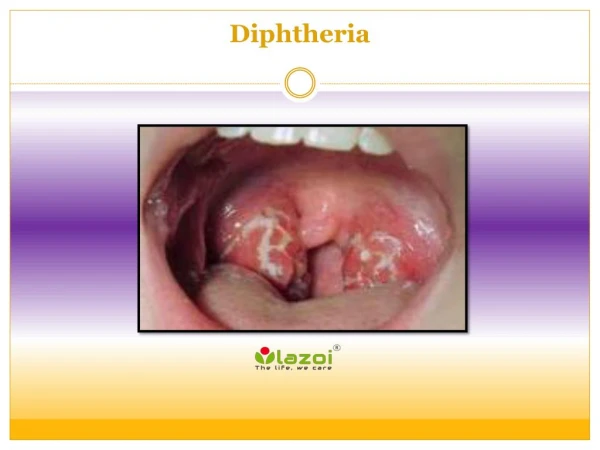
Diphtheria Acute infectious disease characterised by liberation of an exotoxin resulting in: • Formation of greyish / yellowish membrane (“false membrane”) over tonsils, pharynx, or larynx, with well-defined edges. Dr.Harivansh Chopra
Diphtheria • Congestion, Oedema, or Local Tissue Destruction. • Regional lymphadenopathy (Bullneck). • Toxemia. Child with bullneck diphtheria Dr.Harivansh Chopra
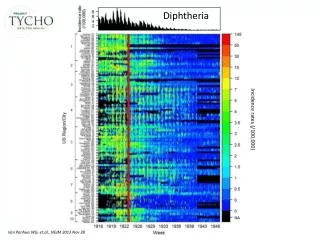
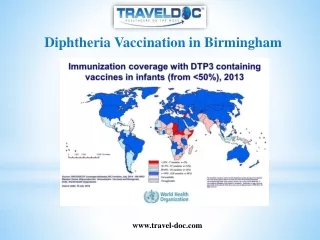
Problem Statement – World • Rare disease in most developed countries owing to vaccination. • Global burden in 2002: • 185,000 DALYs. • 5000 deaths. Dr.Harivansh Chopra
Problem Statement – India Endemic, with declining trend. 99.06% Dr.Harivansh Chopra
Diphtheria – Major Types • Anterior Nasal. • Faucial. • Laryngeal. Dr.Harivansh Chopra
Diphtheria – Other Types • Conjunctival. • Skin. • Genital. Dr.Harivansh Chopra
Diphtheria – Agent Factor • .Corynebacterium diphtheriae. • Gram positive, Non-motile. Dr.Harivansh Chopra
Diphtheria – Agent Factor • .Types – • Gravis. • Mitis. Dr.Harivansh Chopra
Diphtheria – Agent Factor • .Types – • Intermedius. • May be – • Toxigenic. • Non-toxigenic – bacteriophage can convert them into toxigenic. C. diptheriae intermedius Dr.Harivansh Chopra
Diphtheria – Host Factors • Source of infection – • Cases. • Carriers – 95 carriers for 5 cases: • Types – Temporary & Chronic. • May be nasal or throat. • Incidence is 0.1 – 5.0%. Dr.Harivansh Chopra
Diphtheria – Infective Material • Nasopharyngeal secretions. • Discharge from skin lesions. • Fomites – • Throat spatulas. • Utensils. • Toys. • Pencils. Dr.Harivansh Chopra
Period of Infectivity • 14 – 28 days unless treated. • Carriers may remain infective for much longer period. Dr.Harivansh Chopra
Diphtheria – Portal of entry Respiratory Route Non-Respiratory Route Dr.Harivansh Chopra
Mode of Transmission • Droplet infection. • Droplet nuclei. • Through infected cutaneous lesions. • Through – • Milk. • Foods. • Fomites. Dr.Harivansh Chopra
Incubation Period 2 – 6 days. Dr.Harivansh Chopra
Diphtheria – Environmental Factors Transmission favoured in winter season. Dr.Harivansh Chopra
Diphtheria – Clinical Features Anterior Nasal: More common in Infants. • Rhinorrhoea – Discharge may be: • Watery. • Serosanguinous. • Purulent. • Foul-smelling. Dr.Harivansh Chopra
Diphtheria – Clinical Features Anterior Nasal: • White membrane. • Delayed systemic manifestations. Dr.Harivansh Chopra
Diphtheria – Clinical Features Pharyngeal/Tonsillar : • Symptoms: • Sore throat. • 50% have fever. • Few have dysphagia, hoarseness, malaise, or headache. Dr.Harivansh Chopra
Diphtheria – Clinical Features Pharyngeal/Tonsillar : • Signs: • Unilateral or bilateral tonsillar membrane formation, which extends to cover uvula, soft palate, posterior oropharynx, hypopharynx, and glottis. Dr.Harivansh Chopra
Diphtheria – Clinical Features Pharyngeal/Tonsillar : • Signs: • Soft tissue oedema. • Enlarged lymph nodes, resulting in bull-neck appearance. • Effort to remove membrane results in haemorrhage. Dr.Harivansh Chopra
Diphtheria – Clinical Features Laryngeal: • Noisy breathing. • Stridor. • Hoarseness of voice. • Dry cough. • Fever. • May lead to asphyxia. Dr.Harivansh Chopra
Diphtheria – Clinical Features Cutaneous: • Ulcers around mouth and nose. • Ulcers: • Defined border. • Membranous base. Dr.Harivansh Chopra
Diphtheria – Clinical Features Conjunctival: • Affects palpebral conjunctiva. • Presentation: • Oedematous. • Membrane formation. Dr.Harivansh Chopra
Diphtheria – Clinical Features Aural: • Otitis externa. • Discharge: • Persistant. • Purulent. • Foul-smelling. Dr.Harivansh Chopra
Diphtheria – Diagnosis • Specimen: Nasal and throat swab, or any other muco-cutaneous lesion. • Portion of membrane, and underlying exudate submitted. • Laboratory notified to use selective media. Dr.Harivansh Chopra
Diagnosis • Early diagnosis is important. • Diagnosis based on high suspicion in a child with: • Sore throat. • Dyspnea. • Noisy breathing. • Fever. Dr.Harivansh Chopra
Differential Diagnosis Tonsillopharyngeal type: • Acute streptococcal membranous tonsillitis. • Viral membranous tonsillitis. Dr.Harivansh Chopra
Differential Diagnosis Tonsillopharyngeal type: • Herpes tonsillitis. • Thrush. • Infectious mononucleosis. Dr.Harivansh Chopra
Differential Diagnosis Nasal type: • Foreign body in the nose. • Snuffle. • Rhinorrhoea. Dr.Harivansh Chopra
Treatment • Start treatment at earliest on clinical suspicion. • Don’t wait for the laboratory report. Dr.Harivansh Chopra
Treatment – Principles Antitoxins – Neutralising circulating Toxins. Antibiotics – Eradicate Bacteria. Supportive Treatment. Manage Complications. Dr.Harivansh Chopra
Passive Immunisation – Immunoglobulins • ADS of horse origin. • ADS of human origin. Dr.Harivansh Chopra
Dosage of antitoxin (equine) Must be used only after sensitivity test. Dr.Harivansh Chopra
Dosage of antitoxin (equine) Must be used only after sensitivity test. Dr.Harivansh Chopra
Antitoxin Treatment – human • Dose: 0.6 ml/kg body weight Intramuscular (Available as 2ml vial with 300 mg Globulins). • Advantage over ADS (horse origin): • Hypersensitivity absent. • Longer protection. Dr.Harivansh Chopra
Treatment • Antibiotics: • No substitute to anti-toxin. • Stops production of more toxin. • Dosage: • Erythromycin: 40-50mg/kg/24 hrs. divided 6 hourly orally QID X 14 days. Dr.Harivansh Chopra
Treatment • Dosage: • Crystalline Penicillin G: 100,000 – 150,000 IU/kg/24 hrs in 4 – 6 divided doses I.V./I.M. X 14 days. OR • Procaine Penicillin: 25,000 – 50,000 IU/kg/24 hrs in 2 divided doses IM X 14 days. Dr.Harivansh Chopra
Diphtheria Complication – Asphyxia Obstruction of respiratory passage by membrane: • Tachypnea. • Stridor. • Use of accessory muscles of respiration. • Cyanosis. Dr.Harivansh Chopra
Treatment of Asphyxia • Tracheostomy. • Humidified air. Dr.Harivansh Chopra
Diphtheria Complication – Myocarditis • In acute phase. • Toxic cardiomyopathy occurs in approx 10-25% patients and is responsible for 50-60% of deaths. • Usually in 2nd – 3rd week of illness. Dr.Harivansh Chopra
Treatment of Myocarditis • Bed rest, Avoid exertion. • Restrict fluid and salt intake. • Diuretics. • May need sedation and oxygen. • Digoxin in decompensated heart. Dr.Harivansh Chopra
Diphtheria Complication – Neurological involvement • Parallel the onset of primary infection. • Multiphasic in onset: Dr.Harivansh Chopra
Diphtheria Complication – Neurological involvement • Palatal and Pharyngeal paralysis: • Swallowing difficulty. • Nasal voice. • Regurgitation through nose. Dr.Harivansh Chopra
Diphtheria Complication – Neurological involvement Peripheral Neuropathy: • Occurs 1 – 3 months after. • Paraesthesia. • Resolves completely. Dr.Harivansh Chopra
Treatment of Neurological complications • Nasogastric feeding. • Treatment of general weakness. Dr.Harivansh Chopra
Case fatality rate • With Treatment – <5% (Unchanged for the past 50 years). • Without treatment – 10%. Dr.Harivansh Chopra