Download
1 / 95
950 likes | 1.1k Vues
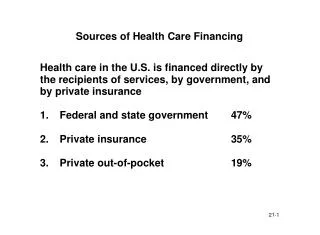
Health Insurance 101: ACA Overview, Update and Q&A South Carolina Health Underwriters Association March 25, 2014 9:00 a.m. – 10:00 a.m. Today’s Focus. ACA Overview, Update and its Impact on South Carolina’s Health Insurance Market Frequently Asked Questions regarding the ACA Q&A Session.

E N D
Health Insurance 101:ACA Overview, Update and Q&ASouth Carolina Health Underwriters AssociationMarch 25, 20149:00 a.m. – 10:00 a.m.
Today’s Focus • ACA Overview, Update and its Impact on South Carolina’s Health Insurance Market • Frequently Asked Questions regarding the ACA • Q&A Session
Key RegulatoryRoles and Responsibilities • South Carolina • License insurance companies • License insurance agents • Review policy forms for health insurance • Review rates charged for health insurance products • Assist consumers with questions or issues related to health insurance • Monitor the SC health insurance market • Federal Government • Implement the ACA • Establish and operate the federally-facilitated exchanges • Certify QHPs • Create and oversee certification of assisters • Determine federal subsidies and issue payments • Enforce coverage mandates • Regulate and oversee the implementation of ACA’s provisions for self-insured plans
The Affordable Care Act’s Enactment Made up of two laws: • The Patient Protection and Affordable Care Act Public Law No. 111-148 Enacted March 23, 2010 As amended by: • The Health Care and Education Reconciliation Act Public Law No. 111-152 Enacted March 30, 2010
Also known as… Health Care Reform PPACA Obamacare Health Care Law
Key Insurance Market Reforms Immediate Market Reforms Effective September 23, 2010* • Restricted Annual Dollar Limits • No Pre-existing Condition Exclusions for Children (Up to Age 19) • No Lifetime Limits • No Rescissions of Coverage/ Appeals Process • Extension of Dependent Coverage to Age 26 • First Dollar Coverage of Preventive Services • Access to ER Services *6 months following PPACA’s enactment date of March 23, 2010. Additional Market Reforms Effective January 1, 2014* • No Annual Dollar Limits • No Pre-existing Condition Exclusions for All • Guaranteed Issue for All • Guaranteed Renewability • Coverage for Individuals Participating in Approved Cancer Clinical Trials • Coverage of Essential Health Benefits *Health Insurance Exchanges also go into effect at this time (more details on Exchanges in later slides). Note: Not all of these provisions apply to grandfathered health plans (more details on later slides).
Changes to Premium Rate Regulation Medical Loss Ratios (MLRs) • 2011 and thereafter • Individual & Small Group: 80% Small Group = 2-50 employees • Large Group: 85% Large Group = 51+ employees Example: An insurer offering individual insurance must spend 80¢ out of every $1 in premium revenues on claims/ health care quality improvements. • State Flexibility: • Can Request Individual Market Waiver (Subject to HHS Approval) • Can Require Higher Minimum MLRs • Rebates required if carriers fail to meet minimum MLR @ end of plan year.
Changes to Premium Rate Regulation Premium Rate Review Effective 7/1/2011 • HHS Secretary to develop process for annual review of “unreasonable” premium increases in consultation with states • Applies to rate increases filed on/ after effective date • Rate filings with a 10% or more increase will be subject to review • Carriers are required to submit to state/ HHS Secretary justification for unreasonable premium increase and post it online Limits on Rate Variations Effective 2014 • Rates for a particular plan/ policy may only vary based on: • Plan/ Policy Type (Individual or Family) • Rating Area (SC has 46 rating areas - one per county) • Age (Age Bands Permissible; 3:1 max ratio) • Tobacco Use (1.5:1 max ratio) • No longer permitted to rate based upon other factors, including: • Sex (male/ female) • Health status • Etc. South Carolina has been deemed as an Effective Rate Review state by HHS.
Health Insurance Exchanges • Two Exchanges: • Health Insurance Marketplace (Individual Market) • Small Business Health Options Program a/k/a SHOP (Small Group Market) • If a state does not establish an Exchange, the HHS Secretary is required to do so in that state. • South Carolina is one of 27 states that have Federally-facilitated Exchanges (FFEs). • 7 states have established Partnership Exchanges. • 17 states (including D.C.) have established State-based Exchanges.
Exchange Basics Must be operated by a governmental agency (state or federal) or nonprofit entity. Can only offer qualified plans to individuals or employers. (Exception: Exchange-certified Stand Alone Dental Plans) Must provide for enrollment periods (initial, annual, special).
Exchange Plans • Qualified Health Plans (QHPs) Must: • Be offered by a carrier licensed and in good standing in the state • Provide Essential Benefits Package (as determined by HHS)* • Agree to offer at least one Silver and one Gold plan • Agree to charge same price on and off of Exchange for same plan • New Issuers/ Options: • CO-OP Plans • Originally intended to provide $6B in funding for establishment of at least one/ state, but reduced by funding cuts to roughly $2B. • 23 states, including South Carolina. • South Carolina’s CO-OP: Consumer’s Choice Health Plan • Multi-State Plans • Office of Personnel Management (OPM) responsible for contracting with carriers that write in multiple states. • In 2014, two MSPP products – one Gold plan and one Silver plan – will be available in the individual market FFE in South Carolina. These are underwritten by BlueCross BlueShield of South Carolina. *State mandates apply if enacted before 12/31/2012. If after that date, state must assume cost of new benefit mandate(s).
Metal Levels Plans are separated into categories, commonly referred to as the Plan Metal Level, based on the percentage the plan pays of the average overall cost of providing essential health benefits to members, aka Actuarial Value (AV). The plan category you choose affects the total amount you'll likely spend for essential health benefits during the year. The percentages the plans will spend, on average, are:
Metal Levels (con’t) Example: A Silver Plan with an actuarial value of 70% means that, on average, the consumer would pay 30% of the costs of all covered benefits through out of pocket cost sharing. The AV is an average of expected costs across a standard population, so any individual could be responsible for a higher or lower percentage of the total costs of covered services for the year, depending on their actual health care needs and the terms of their insurance policy. Off FFE plans will also be assigned a metal level.
Catastrophic Plans Must meet all of the requirements applicable to other Qualified Health Plans (QHPs), but coverage will be slightly less generous than the Bronze level plans. These plans are not required to cover benefits before the plan's deductible is met with one exception: they must cover three primary care visits per year regardless of whether or not the plan's deductible has been met. The monthly premium is generally lower than for other QHPs, but the out-of-pocket costs for deductibles, copayments, and coinsurance are generally higher. Additionally, the federal government has limited enrollment in catastrophic plans. To qualify for a catastrophic plan, you must be under 30 years old OR get a "hardship exemption" from the Health Insurance Marketplace. Finally, federal subsidies (e.g., premium tax credits and cost-sharing reductions) aren't available for catastrophic plans.
Minimum Exchange Functions Health Plans Implement procedures for certification, recertification, and decertification of health plans. Assign a rating to each health plan. Consumer Information Operate a toll-free hotline. Maintain Internet website with standardized information. Utilize standardized format for presenting options. Make available a calculator to determine the actual cost of coverage after subsidies. Establish a Navigator program.
Minimum Exchange Functions (con’t) Eligibility Determinations • Inform individuals of eligibility for Medicaid, CHIP, or other applicable state or local public programs (“No Wrong Door”) • Certify exemptions from individual mandate. • Grant a certification attesting that the individual is not subject to the coverage mandate because: • there is no affordable option available; or • the individual is exempt from the mandate. • Transfer to the Treasury information on exempt individuals and employees eligible for tax credit. • Provide to each employer the names of employees eligible for tax credit.
Certification of QHPs • Qualified health plans must meet minimum requirements in order to be certified and maintain certification. • ACA requires this criteria include requirements relating to: • Marketing • Network Adequacy • Availability of in-network and out-of-network providers • Access to essential community providers for low-income/ medically-underserved • Clinical Quality Accreditation by HHS-recognized organization • Quality Improvement Strategies • Uniform Enrollment Form • Standardized Format for Presenting Plan Options
Exchange Subsidies Individual Subsidies • Eligibility is based on Household Income as a % of Federal Poverty Level (FPL) • Premium Subsidies • Tax credit that is taken in advance, so that the government pays a portion of your monthly premium • Must select a Metal Level Plan (not available for Catastrophic Plans) • 100% - 400% FPL • $11,490 - $45960 for individuals • $23,550 - $94,200 for a family of 4 • Reduced Cost Sharing • Lowers the out of pocket costs (e.g., deductibles, coinsurance, and co-pays) that insureds must pay • Must select a Silver Plan • 100% - 250% FPL • Max of $28,725 for individuals or • $56,875 for a family of 4 Small Business Tax Credits • 2010 - 2013 • Up to 35% of employer contribution for employees’ health insurance • 2014 and thereafter • Up to 50% of employer contribution • Must be Exchange plan • Limited to 2 years • Eligible Businesses • 25 or fewer employees • Average wages of $50,000 or less • Employer contributes 50%+ of premium
Off the Exchange vs. On the Exchange Federal subsidies for individuals and small businesses are only accessible if purchasing a QHP through the Exchanges More carriers and plan types will be available outside of the Exchanges in 2014
Individual Market OptionsIndividuals, Families, and Self-Employed
Employer Impact • ACA’s impact will vary depending upon: • The size of the employer • Whether the employer currently offers health insurance • Current state insurance laws and regulations • Whether the plan is grandfathered or “grandmothered” or ACA compliant.
Provisions Applicable to All Employers • All health plans must comply with the following including grandfathered plans: • No lifetime caps on coverage • No annual limits on essential health benefits • Expanded dependent coverage to age 26 • Restrictions on the ability to rescind a policy • Limits on FSA contributions • Medical Loss ratio rebates • No pre-existing condition exclusions • Summary of Benefits and Coverage
ACA’s Individual Impact • Depends upon: • Whether the individual has minimum essential coverage through another plan including • TriCare • Medicare • Qualifying Employer Sponsored Insurance Coverage • Qualifying Individual Health Insurance Coverage • the size of the employer • Portions of the ACA has been delayed for large and mid-size employers • Whether existing coverage is grandfathered, grandmothered or other • Age • Uninsured • All Americans must have some form of health insurance by March 31, 2014 or face a penalty.
Off the Exchange Note: the companies/ plans highlighted in grey and italicized have not yet been approved.
“Grandfathered” Plans A grandfathered health plan is a plan that has existed continuously since before March 23, 2010, without significant changes in the plan. Grandfathered plans aren’t subject to many of the requirements of the ACA, such as the requirement that plans cover essential health benefits. Grandfathered plans that make certain changes, such as major increases in their cost-sharing (e.g., coinsurance, deductibles, copayments), or eliminating benefits, may lose grandfathered status. Employer-sponsored plans that significantly raise the employee share of the premium also could lose grandfathered status. A plan must indicate in the plan materials if it is a grandfathered plan. Also, consumers can check with their insurance company or employer. Note: the State Health Plan is a grandfathered plan.
“Grandmothered” Plans • On November 14, 2013, President Obama announced that States could decide whether to allow small group and individual health insurance policies existing on October 1, 2013 to be renewed for a policy year starting between January 1, 2014 and October 1, 2014. To give consumers the most options, some states allowed health insurers to offer the renewal option. South Carolina was one of them. • Essentially, for consumers these are the choices in the market for SC consumers: • “Grandfathered 2010” health plans. The federal law specifies conditions for grandfathered plans that existed in March 2010. Grandfathered health plans cannot be sold on the online marketplace or the federally-facilitated exchange (FFE). Many people will not have access to this option because their policies changed after March 2010. • “Transitional renewal plans” also called “Grandmothered” health plans. These plans must have been in existence on October 1, 2013 and renewed prior to October 1, 2014. They include some but not all of the ACA features. Transitional or “Grandmothered” health plans cannot be sold on the online marketplace or the FFE. These plans will be subject to updated premium rates. You may only apply for a renewal policy, not a newly issued policy. On March 5, 2014, the federal government announced that it was extending the transitional renewal policies. • “Fully compliant new 2014 ACA” plans. Non-Grandmotheredor nongrandfathered plans must include all ACA features, including the 10 Essential Health Benefits. Fully compliant ACA plans will be sold on and off the FFE.
Implementation of Initial Transitional Policy (November 2013) Under this federal announcement, if certain specified conditions are met, health insurance coverage in the individual or small group market that is renewed for a policy year starting between January 1, 2014 and October 1, 2014 will not be considered to be out of compliance with the following federal market reforms which are included in the Public Health Service Act and scheduled to take effect for plan or policy years starting on or after January1, 2014: • PHSA §2701 (relating to fair health insurance premiums); • PHSA §2702 (relating to guaranteed availability of coverage); • PHSA §2703 (relating to guaranteed renewability of coverage); • PHSA §2704 (relating to the prohibition of pre-existing condition exclusions or other discrimination based on health status) with respect to adults, except with respect to group coverage; • PHSA §2705 (relating to prohibitions on discrimination against individual participants and beneficiaries based on health status), except with respect to group coverage; • PHSA §2706 (relating to non-discrimination in health care); • PHSA §2707 (relating to comprehensive health insurance coverage); and • PHSA §2709, as codified at 42 U.S.C. §300gg-8(relating to coverage for individuals participating in approved clinical trials). • A number of states opted to implement the November 5 transitional policy. South Carolina was one of those states. Others did not. • Bulletin 2013-12 sets forth the South Carolina’s guidance on this issue.
ACA Market Impact? No one knows really. Results vary among the states. For example, California and New York are viewed or “appear” to be more competitive post-ACA. In contrast, CT and WA markets are viewed as less competitive. In CT, it is reported that two of the largest carriers are not participating in the state’s exchange. The Kaiser Family Foundation has published a report on this issue. The report examines the markets in seven states. South Carolina is not one of the them. Has competition increased in SC? Hard to say… Let’s look at the numbers.
SC Enrollment Numbers as of March 15, 2014 • Number of SC citizens that have secured coverage through the FFE: 43,229. These individual have selected coverage and PAID their premium. This number may differ from other numbers you may see that report the number that have selected coverage through the FFE. • This number represents 64% of the individuals that have gotten through the application, eligibility determination and plan selection process in order to enroll • Percentage of the 43,229 receiving a federal subsidy is: 88.69% • Average age of the individual securing coverage through the FFE is 44.50 • Average age of the individuals who have secured coverage in the market outside the FFE is 35.71 • The DOI will update these numbers after March 31st the last day of open enrollment for 2014.
ACA Market Issues to Date • Difficulty enrolling into the plans offered on the FFE. Some complain that it takes too long and that the premium quoted by healthcare.gov may not be the same as that quoted by the company. Companies say that healthcare.gov is quoting the premium with the subsidy and the applicant may not qualify for the subsidy. • Concerns about the restricted networks • Some plans offer exclusive provider networks • Network adequacy is one of the issues that CMS will be looking into for this next round of QHP applications • Consumers are complaining that they are waiting to hear from the companies. When they call the companies they are told to contact healthcare.gov when the call healthcare.gov, they are told to call the company. • Some consumers have had coverage lapse due to the communication issues between the company and healthcare.gov.
Who can purchase a plan through the FFEs? In South Carolina, any individual or family who wants to may buy coverage through the Health Insurance Marketplace. The only people who can’t are those who aren’t legally in the United States or who are incarcerated (other than pending disposition of charges). Small employers (employers with fewer than 50 employees) may purchase health insurance for their employees through the Small Business Health Options Program (SHOP Exchange). Self-employed individuals and businesses with only one employee may access coverage through the individual market (Health Insurance Marketplace or outside of the FFE). Note: Just because you can purchase a plan through the FFEs does not mean you will qualify for a subsidy.
When will consumers be able to enroll in plans through the Health Insurance Marketplace? The initial open enrollment period ends on March 31, 2014. Individuals who do not have coverage as of that date may be subject to a tax penalty.
When will consumers be able to enroll in plans through the Health Insurance Marketplace? (cont’d.) • Consumers may also be eligible to enroll in coverage at times other than during the open enrollment period. • There are special enrollment periods for individuals or families if they experience a “triggering event.” • Some examples of triggering events include: (1) loss of minimum essential coverage; (2) gaining or becoming a dependent; (3) newly gaining citizenship; and (4) being enrolled if a plan through the exchange without tax credits and then becoming newly eligible for tax credits. • In future years, open enrollment will be each year between October 15 and December 7. During this time, consumers will be able to change plans, change insurance companies or stay with the plan they have if it is still available. This will not be the open enrollment period next year. • Unlike the Health Insurance Marketplace (individual FFE), open enrollment for the SHOP will be year-round for most small employers.
Proposed Open Enrollment Dates for 2015 • Open Enrollment: November 15, 2014 through January 15, 2015 are the proposed dates • Insurers will have to submit their products to the Department for review by May 26, 2014-June 27, 2014 • Insurers interested in being a QHP (i.e., selling products on the exchange) must submit their application by that deadline as well • September 4 is the final QHP submission date • September 20 is the data lock-down date • Contract notifications are sent to issuers in October 2014
How can a consumer prepare for plan selection/ enrollment? There are a number of steps consumers can take to prepare. Healthcare.gov has suggestions for things consumers should be thinking about in preparation for enrolling in a plan. Consumers who do not currently have health insurance coverage should find out if help might be available now through existing programs or because of changes that are already in effect from the ACA. For example, a parent’s plan may cover young adults under age 26. Consumers can also contact an insurance agent or broker for help. Consumers can also check with employers to find out whether they intend to offer health insurance coverage in the future or whether the coverage they currently offer meets the minimum level for complying with the law’s requirement to avoid paying a penalty. Insurance companies must notify policyholders if their plan does not meet ACA requirements (i.e., non-grandfathered health plans that will not be renewed on/after . Finally, consumers can start gathering basic information about household income, such as their 2012 tax return if they filed one, or other income information (necessary to determine eligibility for federal subsidies).
How do the metal levels help consumers compare plans? The tiers are a way to categorize plans based on “actuarial value”. Plans within each tier (catastrophic, bronze, silver, gold, and platinum) have similar actuarial value, even if they cover different benefits or have different types of cost-sharing. While all metal level plans in a given tier must cover essential health benefits, the details of their coverage (such as how many physical therapy visits are covered or which prescription drugs are covered) may be different. Not all plans in the same tier have the same benefits or cost sharing requirements. Some plans may offer benefits in addition to the essential health benefits. Plan types can also vary within a given tier and on v. off the FFEs. Carriers writing in South Carolina have filed a variety of plans, including PPOs, EPOs, POS, and HMOs.
What services/benefits must be covered by plans? What are essential health benefits? • After January 1, 2014, almost all plans sold in the individual and small group market, including those sold through the Health Insurance Marketplace and the SHOP exchange, as well as plans sold in the market outside the exchange, must cover, at a minimum, a comprehensive set of benefits known as essential health benefits. These essential health benefits include the following: • Ambulatory patient services • Emergency services • Hospitalization • Maternity and newborn care • Mental health and substance abuse disorder services, including behavioral health treatment • Prescription drugs • Rehabilitative and habilitative services and devices • Laboratory services • Preventive and wellness services, including chronic disease management • Pediatric services, including oral and vision care • Note: grandfathered plans (both individual and group) don’t have to include EHBs.
How can a consumer find out the details about what a particular plan covers? All individual and small group plans (excluding grandfathered plans) with an effective date on or after January 1, 2014 will cover essential health benefits. To learn if a specific benefit is covered, and at what level, check a plan’s Summary of Benefits and Coverage (SBC). An SBC is a uniform document that includes details about what a plan does and doesn’t cover. It also includes information about what kinds of costs a consumer can expect to pay out-of-pocket, such as copayments, coinsurance, and deductibles. An SBC comes with plans offered through the exchange and in the market outside the exchange. It gives information in the same way for every plan to make it easier to compare plans. The SBC forms are on the federal government’s website at www.healthcare.gov, or from an agent or broker for plans offered in the market outside the exchange. Consumers can read more about the Summary of Benefits and Coverage here: http://www.cms.gov/CCIIO/Programs-and-Initiatives/Consumer-Support-and-Information/Summary-of-Benefits-and-Coverage-and-Uniform-Glossary.html
Can a person remove benefits from a plan? What if a consumer does not need them all? No, benefits cannot be removed from a plan, although a consumer may be able to add extra coverage. This is true for grandfathered and non-grandfathered plans. Even though a person may not need every benefit on a plan, coverage is required for all of these benefits in order to share risk across a broad pool of consumers and make sure all benefits are available for everyone. This also helps to protect people from risks they cannot always foresee across their lifetimes.
Can a person’s health condition affect their coverage? Generally, the answer is “No.” Under the ACA, health insurance companies can no longer put limits on coverage based on a person’s health condition, often called “pre-existing condition exclusions,” nor can they charge a higher premium because of a person’s health condition. These protections apply regardless of whether a person purchases coverage through the exchange or outside the exchange. Note: The prohibition on pre-existing condition exclusions does not apply to individual grandfathered plans (but does apply to group grandfathered plans).
Can an insurance company charge smokers more than non-smokers? Under the ACA, health insurance companies can ask about tobacco use before enrolling a consumer in a plan, and can then charge consumers who use tobacco products a higher premium. Consumers in group plans may avoid this extra charge by enrolling in a tobacco cessation program.
What are preventive benefits and how are they covered? • Preventive benefits are designed to keep people healthy by providing screening for early detection of certain health conditions or for helping to prevent illnesses. The ACA requires that plans cover many preventive services with no out-of-pocket costs (meaning no deductibles, co-payments, and coinsurance) for all plans beginning September 23, 2010. Some of these covered preventive services are: • Colorectal cancer screenings, including polyp removal for individuals over age 50 • Immunizations and vaccines for adults and children • Counseling to help adults stop smoking • Well-woman checkups, as well as mammograms and cervical cancer screenings • Well-baby and well-child exams for children • Unless an insurer does not have an in-network provider to perform a particular preventative service, plans are permitted to charge for these preventative services when performed by an out-of-network provider. • For more information on preventive services, see healthcare.gov and do a search for preventive services.
How does a consumer find out what drugs are covered by a plan? Health plans maintain lists of which drugs are covered and which are covered at the lowest costs. These lists are called formularies. Drug cost-sharing is often “tiered,” that is, consumers pay less for a generic drug, more for a brand name drug, and sometimes even more for a non-preferred brand name drug. Consumers should review the formularies in any plan selected to make sure they meet their prescription drug needs and they know what cost sharing is required for any given drug. For plans that use formularies, the SBC includes an internet address (or similar contact information) for obtaining information on the plan’s drug coverage. Consumers can call their health insurer for help.