Vaginal Discharge
E N D
Presentation Transcript
DEFINITIONRunning of white substance and the. than bloodNB: Normally the vagina and the introitus are kept moist by the following: 1. Bartholin gland play the most important role in the lubrication of vaginal introitus. It secrete a thick mucus which is increased during sexual intercourse.
2. In the periurethral region of the visible are situated Skerie's ducts which contribute to the lubrication of the vulval structures. 3. Although the vagina is itself devoid of glands its surfaces is moistened by the secretion of the cervical glands and to much less extent by transudation from its own surface.
CausesI. Physiological causes: pelvic Congestion : 1. During pregnancy 2. Chronic constipation 3. Sedentary life 4. At the time of ovulation 5. Emotional and sexual upset
II. Pathological Causes: 1. INFLAMMATORY CONDITION: Vulvitis, vaginitis, cervical erosion, tuberculous, endometritis, puerperal sepsis, chronic salpingo-oophritis and pelvic abscess draining vaginally 2. NEOPLASTIC CONDITION:-Infected cervical polyp Malignant neoplasia in the lower genital tract
3. FOREIGN BODY :a. Intrauterine contraceptive device b. Neglected pessaryc. Neglected tampoon - vaginal diaphragm or contraception sponge 4. VAGINAL ADENOSIS: Islands of mullerian glandular epithelium can be detected in an area which is lined by st. sq. epithelium
5. INTERMITTENT HYDROSALPINX 6 . Ascitis Fluid 7. SMALL VVF OR SI8. ANTE-PARTUM R.M.
Diagnosis:I. History - Onset. duration and amount of discharge-- - Character of discharge white ----} pelvic congestion ~ mucoid ----> cervical erosion ~ purulent ----) infection offensive ----> pyometra, retained FB serous ----> early malignant blood stained ----) senile vaginitis or malignant tumour
ASSOCIATED SYMPTOMS: itching (monilial or trichomonasvaginitis) dysuria - gonoccal infection .previous medication " menstrual troubles last abortion or labour
Examination: -General examination for anaemia or cachexia- Abdominal ex.: for abdominal swelling or tenderness - Local examination Inspection of the vulva from sign of urethritis and BartholinitisMaking of the urethra and any discharge comes should be examined for gonococcal- Speculum examination * The amount, consistency, character and odour of discharge * The vaginal wall and the c.ervix are inspected .' for ulceration, .. : polyps or cancer - Bimanual ex to exclude uterine or adnexal causes
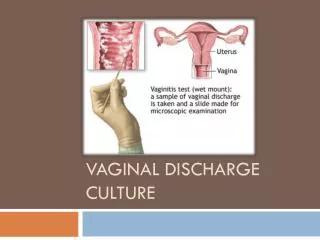
III. Investigation1. Three drops of the discharge are taken, then first for wet smear (a drop of saline is added and examined in microscope). The second for dry smear (direct film is prepared and stained with gum stain) and the third for culture and sensitivity 2. Biopsy is taken from any detectable lesion 3. Serological test 4. Tests for diagnosis of gonorrhea 5. Cytological smear for early detection of cervical smear6. In children, x-ray is done for detection of any· radio-opaque L.B. in the vagina
TreatmentTreatment of the cause Non-infective vaginal discharge is managed by - Minimize pelvic congestion by active exercises and active life - Pelvic decongestant as glycerineicthyolpessaries- Cleanliness
MonilialVaginitisCAUSATIVE FUNGUS: Candida albican. [gm + veunicellula. Organism reproduce by budding, spore forming, characterized by pseudo hyphae formation.
Predisposing Factors: Acidic PH of the vagina (4-5) Pregnancy as vaginal PH more acidic Oral contraceptive pills Antibiotic ---) alternation of normal vaginal flora Diabetes due to high glucose in blood and urine Corticosteroid and other immunosuppressive drugs Clinical manifestation of monilia increased before period and decreased during and after menses
Mode of InfectionTransformed from carrier state into active state. SymptomsItching Vaginal discharge
Signs:- Sign of scratching and acute inflammation in the vulva - Vagina shows white patches adherent to the mucera its removal leaves bare area with bleeding [ - Vaginal discharge ---> scanty, thick, white curdy with offensive odourInvestigation:(1) Wet smear: A drop vaginal discharge is mixed with drop of KoH 10% and examined microscopically (2) Direct film is prepared and stained with M.S. the organism identified by long slender filament ends in small buds
Treatment1.Nystatin vaginal tab Oral Tabnystatin cream2. Gention violet 1% aqueous solution local application : 3. ImidazolederviathMiconazole - very supp Tioconazol - vaginal tab ~ Ketoconazol - vaginal tab ~ Clotrimazole4. Na bicarbonate vaginal douches ---> decreased vaginal acidityControl of diabetes
TrichomonasVagincalCAUSITIVE PARASITE: Trichomonasvigincalis: [motile, flagellate, 10-15 micron in dialmeter, oval or bear shaped, 4 anterior flagellaeaxostyle traversing the body, ends in small spiky. The nucleus is situated in the b.oad end of parasite.
There are 3 types of trichomonas: 1. Trichomonasvaginalis present in vagina 2. Trichomonasbuccalis present in mouth 3. Trichomonashomanis present in rectum and anal canal
Mode of InfextionSexual contact Bad sexual hygiene - infected cloths, baths of or gloves Symptoms:1.Vaginal discharge, thin coplus foamy greenish yellow in colour and offensive 2. Dyspneadyspareunia due to local cystitis 3. itching4. Frequency in micturation due to local cystitiisSign :1. Characteristic vaginal discharge2. Vaginal mucosa is congested and granular (Strawberry vaginal
INVESTIGATION:1.Wet film drop of vaginal discharge is mixed with drop of warm saline and examined microscopically 2. Dry film ---> direct film is prepared and stained with Leishman stain 3. CultureKupferberg'swhittington medics '" TREATMEIT: 1. Metronidazole (Flagyl) 3 times for 7-10 days 2. Tinidazole (fasigyn) 2 gm single dose 3. During pregnancy ---} clotrimazolevagincalpessary
PRURITISDefinitionIt is termed used to describe a sensation of irritation from which the patient attempts to gain relief by scratching. CAUSES1.Vaginal discharge ---> profuse or persistent vaginal discharge may lead to irritation of the vulval skin as trichomonasvaginitis and monilial vulva-vaginitis2.Urinary conditions: Glycosuria3. Rectal condition, threadworm infestation 4. Diseases of the vulval skin: chronic epithelial dystrophies eczema, seborrhoeic dermatitis and psorIasis5. Parasitic condition: pedculosis or scabies6. Psychological (Neurodermatitis)
Diagnosis: A. History1. The onset, site and duration of itching 2. Presence or absence of vaginal discharge 3. Generalized alliergic disorders 4. Past for family history of diabetes B. ExaminationGeneral examination ---> anaemia or jaundice Local examination ---> vulvitis or vaginal discharge
C. Investigation: 1. Urine for sugar or bile pigment 2. Blood for Hb% glucose tolerance test, serum bilirubin level 3. Bacteriological examination of vaginal discharge' 4. Biopsy from any abnormal vulval lesion 5. Fractional meal test for achlorhydria
TREATMEIIT: 1. Treatment of the cause 2. General measure: sedatives, antihistamines, estrogen in past menopausal female 3. Local treatment Local cleanliness Hydrocortisone iotion or cream Estrogen cream in postmenopausal women ~ Antihistaminic cream or lotion Local anesthetic spray Antifungal cream Ultraviolet light
4. Surgical measures (rare) S.C. infection of 95% alcohol into the vulva S.C. infiltration with local anesthetic or hydrocortisone Circular incision around the vulva to cut the nerve fibresSimple vulvectomy in resistant cases
Chronic Episthelial Dystrophies of the VulvaDIFINTION: Disorders in the epithelial growth and nutrition which result in white surface lesion of the vulva. This Include:1. Atrophic type (lichen sclerosis) 2. Hypertrophic type (leukoplakia) e' or 'eoutatypia3. Mixed type with or without atypiaAtrophic type (lichen sclerosis) Develop after age of menopause but may occur at any age.
CAUSES IF VULVAL DYSTRIIIIIES : 1. Chronic irritation 2. Hormonal defficiency3. Alternation of hormonal receptivity 4. Disturbance of CT factor 5. Chalone: tissue protein with hormonal like action It is secreted by the epjdermis and inhibiteepjthelial proliferation. Increased the concentration of chalone result in atrophic changes. While decreased the concentration of chalone result in hypertrophic changes.
Clinical Picture: 1. Severe itching 2. Itching of skin ---> scratching, exocriation, secondary infection MANAGEMEIIT: Advise the patient to avoid use of pe.futnes, douches and even take shower, I. Advice patient to use cotton pants 3. Wash the vulva by none irritant soap 4. Biopsyfor histopathological study and treatment