Vaginal Discharge
Vaginal Discharge. Jan 2014. Q1. A 24-year-old woman presents due to an itchy vulva and pain during sex. She also mentions a green, offensive vaginal discharge for the past 2 weeks. What is the most likely diagnosis? Candida Bacterial vaginosis Gonorrhoea Trichomonas vaginalis Chlamydia

Vaginal Discharge
E N D
Presentation Transcript
Vaginal Discharge Jan 2014
Q1. A 24-year-old woman presents due to an itchy vulva and pain during sex. She also mentions a green, offensive vaginal discharge for the past 2 weeks. What is the most likely diagnosis? Candida Bacterial vaginosis Gonorrhoea Trichomonasvaginalis Chlamydia Q2. A 30-year-old woman presents with a white, malodorous vaginal discharge. There is no associated itch or dyspareunia. A diagnosis of bacterial vaginosis is suspected.Overgrowth of which one of the following organisms is most likely to cause this presentation? Lactobacilli Trichomonas Candida Mycoplasmahominis Gardnerella
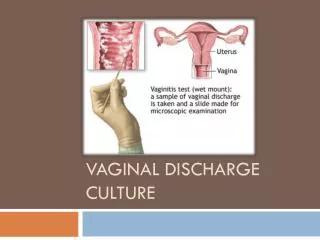
Vaginal discharge • Vaginal discharge is a common presenting symptom and is not always pathologicalCommon causes • -physiological • -Candida • -Trichomonasvaginalis • -bacterial vaginosis • Less common causes • -Chlamydia and Gonorrhoea can cause a vaginal discharge this is rarely the presenting symptoms • -ectropion • -foreign body • -cervical cancer
Q3.A 41-year-old female is diagnosed as having Trichomonasvaginalis. What is the most appropriate management • Clotrimazolepessary • Oral doxycycline • Advice regarding hygiene and cotton underwear • Oral itraconazole • Oral metronidazole Q4. Which one of the following features is least consistent with Trichomonasvaginalis • Strawberry cervix • Vulvovaginitis • Vaginal pH < 4.5 • Urethritis in men • Frothy green discharge
Trichomonasvaginalis • Trichomonasvaginalis is a highly motile, flagellated protozoan parasiteFeatures • vaginal discharge: offensive, yellow/green, frothy • vulvovaginitis • strawberry cervix • pH > 4.5 • in men is usually asymptomatic but may cause urethritis • Investigation • microscopy of a wet mount shows motile trophozoites • Management • oral metronidazole for 5-7 days, although the BNF also supports the use of a one-off • dose of 2g metronidazole
Q5.A 25-year-old woman attends clinic for her regular cervical smear test. She is not complaining of any symptoms. • The results of the smear show no evidence of dysplasia but the pathologist notes the presence of fusiform protozoa in the specimen. • Which of these is the most likely diagnosis? • Bacterial Vaginosis • Candida Infection • Group A Streptococcusinfection • Herpes simplex virus infection • Trichomonasvaginalis infection • Q6. A 23-year-old female presents 16 weeks into her pregnancy with a vaginal discharge. Further investigation confirms infection with Chlamydia trachomatis. • Which of the following is the most appropriate treatment for this patient? • Azithromycin • Cotrimoxazole • Doxycycline • Erythromycin • Metronidazole • Current UK guidelines recommend three different options in pregnancy: • Erythromycin 500 mg QDS for 7 days or BD for 14 days • Amoxicillin 500 mg TDS for 7 days • Azithromycin 1 g stat - the BNF cautions that this should only be used if there are no
Q7.A 31-year-old woman presents as she has noted an offensive, fishy vaginal discharge. She describes a grey, watery discharge. What is the most likely diagnosis? • Trichomonasvaginalis • Candida • Chlamydia • Bacterial vaginosis • Physiological discharge • Q8 .A 30-year-old woman presents with a week long history of an offensive smelling greenish-yellow vaginal discharge with associated vulval itching. She does not complain of lower abdominal pain. • She has not been seen by you personally at the clinic and has social problems with frequent episodes of homelessness. She is unkempt and admits to sleeping on the streets. She refuses your request that she should be seen at the local genito-urinary medicine (GUM) clinic. Her scant records are full of "did not attend" entries. Examination reveals a greenish-yellow discharge but is otherwise unremarkable. • Which of the following is the most appropriate approach for this woman? • Admit to hospital • Empirically treat with ciprofloxacin, azithromycin, metronidazole and clotrimazole • Empirically treat with ciprofloxacin only • Routine referral to gynaecology • Take a swab and ask patient to return in one week for the results
Bacterial vaginosis • Bacterial vaginosis (BV) describes an overgrowth of predominately anaerobic organisms such as Gardnerellavaginalis. This leads to a consequent fall in lactic acid producing aerobic lactobacilli resulting in a raised vaginal pH.Whilst BV is not a sexually transmitted infection it is seen almost exclusively in sexually active women.Features • vaginal discharge: 'fishy', offensive. There is no associated soreness, itching or irritation • asymptomatic in 50%. • There may be a white, homogenous discharge coating the walls of the vagina and • vestibule but usually no signs of inflammation • Amsel's criteria for diagnosis of BV - 3 of the following 4 points should be present • thin, white homogenous discharge • clue cells on microscopy • vaginal pH > 4.5 • positive whiff test (addition of potassium hydroxide results in fishy odour)
Management • oral metronidazole for 5-7 days • 70-80% initial cure rate • relapse rate > 50% within 3 months • the BNF suggests topical metronidazole or topical clindamycin as alternatives • Risk factors for BV include: • Vaginal douching • Recent change of sex partner • Smoking • Receptive cunnilingus • Black ethnicity, and • The presence of other infections such as Chlamydia or herpes.
Treatment is indicated for symptomatic women and women undergoing some surgical procedures. the recommended regimes are: • Metronidazole 400 mg twice daily for 5-7 days • Metronidazole 2 g single dose • Intravaginalmetronidazole gel (0.75%) once daily for 5 days • Intravaginalclindamycin cream (2%) once daily for 7 days • Alternative regimens include: • Tinidazole 2 g single dose (A), or • Clindamycin 300 mg twice daily for 7 days (A).
Q9 A 28-year-woman presents with a vaginal discharge. This is clear, intermittent and has been present for a number of months. She has no other symptoms and is in a stable relationship. • With respect to the discharge which one answer is true? • (Please select 1 option) • The most likely cause is a physiological discharge • The most likely cause is bacterial vaginosis • The most likely cause is candidiasis • She should be screened for STI • With these symptoms a speculum and cervical swab is indicated • Q10. A 30-year-old woman in a stable relationship is complaining of a vaginal discharge. There is no irritation but a fishy odour. • Swabs are all negative. She is allergic to metronidazole. • What is the best option for treatment? • Clindamycin cream • Clotrimazole cream • Oral co-amoxiclav • Oral erythromycin • Oral fluconazole
Q10.A 21-year-old woman with persistent dysuria tests positive for Chlamydia. She agrees for referral to GUM for contact tracing. Who should be contacted? • All partners from the 3 months prior to the onset of symptoms • All partners from the last 6 months or the most recent sexual partner • All partners from the last 3 months or the most recent sexual partner • All partners from the last 12 months or the most recent sexual partner • All partners from the 4 weeks prior to the onset of symptoms • Chlamydia - partner notification: • symptomatic men: all partners from the 4 weeks prior to the onset of symptoms • women + asymptomatic men: all partners from the last 6 months or the most recent sexual partner
Q11.What is the most appropriate antibiotic to treat uncomplicated Chlamydia infection in a 21-year-old female who is not pregnant? • Erythromycin • Ciprofloxacin • Metronidazole • Cefixime • Azithromycin • Q12.A 30-year-old man comes to surgery. He has been handed a slip from an ex-girlfriend stating she has tested positive for Chlamydia. He last slept with her 2 months ago. He has no symptoms of note, in particular no dysuria or discharge. What is the most appropriate management? • Reassure symptoms would have presented by now • Offer antibiotic therapy • Offer Chlamydia testing and antibiotic treatment immediately without waiting for the results • Offer Chlamydia testing and antibiotic treatment if positive • Notify public health
Chlamydia • Chlamydia is the most prevalent sexually transmitted infection in the UK and is caused by Chlamydia trachomatis, an obligate intracellular pathogen. • Approximately 1 in 10 young women in the UK have Chlamydia. • The incubation period is around 7-21 days, although it should be remembered a large percentage of cases are asymptomaticFeatures • asymptomatic in around 70% of women and 50% of men • women: cervicitis (discharge, bleeding), dysuria • men: urethral discharge, dysuria • Potential complications • epididymitis • pelvic inflammatory disease • endometritis • increased incidence of ectopic pregnancies • infertility • reactive arthritis • perihepatitis (Fitz-Hugh-Curtis syndrome)
Investigation • traditional cell culture is no longer widely used • nuclear acid amplification tests (NAATs) are now rapidly emerging as the investigation of choice • urine (first void urine sample), vulvovaginal swab or cervical swab may be tested using the NAAT technique • Screening • in England the National Chlamydia Screening Programme is open to all men and women aged 15-24 years • the 2009 SIGN guidelines support this approach, suggesting screening all sexually active patients aged 15-24 years • relies heavily on opportunistic testing
Management • Doxycycline(7 day course) or azithromycin (single dose). • The 2009 SIGN guidelines suggest azithromycin should be used first-line due to potentially poor compliance with a 7 day course of doxycycline • if pregnant then erythromycin or amoxicillin may be used. • The SIGN guidelines suggest considering azithromycin 'following discussion of the balance of benefits and risks with the patient’
Q13.A 32-year-old woman complains of lower abdominal pain/ pelvic pain over the last five days. She also has a raised temperature. She had an IUCD inserted three weeks ago. A pregnancy test is negative, she has a small amount of vaginal discharge, and she has white blood cells present on dipstick test of her urine. What is the most likely cause of these symptoms in this patient? Ectopic pregnancy Pelvic inflammatory disease (PID) Ruptured ovarian cyst Urinary tract infection A 24-year-old female attends complaining of an offensive frothy yellow vaginal discharge with associated vulva itch, and dysuria. Pelvic examination reveals punctuate mucosal haemorrhages on the cervix. What is the most appropriate treatment regime based on the history and clinical examination? Oral azithromycin 1 g as a single dose Oral doxycycline 100 mg BD for seven days Oral fluconazole 150 mg single dose Oral metronidazole 400 mg BD for seven days