Background and Significance
Population Pharmacokinetics of Dexmedetomidine in Infants Following Open Heart Surgery Felice Su MD, Susan C. Nicolson MD, Jeffrey S. Barrett PhD, Peter C. Adamson MD, David S. Kang BS, Rodolfo Godinez MD PhD, Athena F Zuppa MD MSCE

Background and Significance
E N D
Presentation Transcript
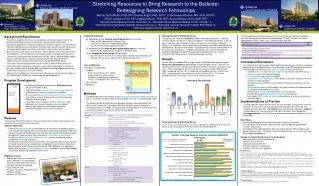
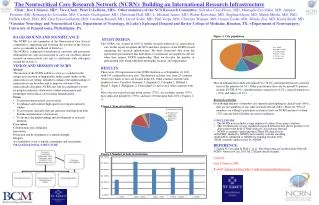
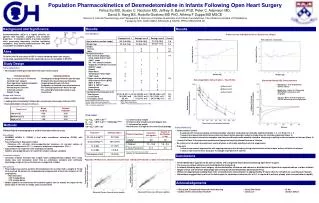
Population Pharmacokinetics of Dexmedetomidine in Infants Following Open Heart SurgeryFelice Su MD, Susan C. Nicolson MD, Jeffrey S. Barrett PhD, Peter C. Adamson MD, David S. Kang BS, Rodolfo Godinez MD PhD, Athena F Zuppa MD MSCE Division of Clinical Pharmacology and Therapeutics & Divisions of Cardiac Anesthesia and Critical Care Medicine, The Children’s Hospital of Philadelphia Funded by NIH, GCRC #MO1-RR-00240 & NICHD, PPRU #HD037255-09 Semi-logarithmic Concentration – Time Profile ● Dose Level 1 ■ Dose Level2 ▲ Dose Level 3 Dexmedetomidine Plasma Concentration (pg/mL) Time from end of infusion (minutes) Results Background and Significance Results C. C. Demographics Dexmedetomidine (DEX) is a highly selective α2-agonist with hypnotic, analgesic and anxiolytic properties. In intubated adults, it provides sedation while preserving respiratory function facilitating extubation. Only limited pharmacokinetic (PK) data is available for pediatric patients. Pattern of Inter-individual Error in Clearance vs. Weight Without allometric relationship With allometric relationship Aims Inter-individual Error Inter-individual Error • To define the PK and safety of DEX in infants following open heart surgery • To develop a population PK model exploring sources of variability in DEX PK Study Design Patient population • 36 evaluable infants post-operative from open heart surgery Weight (kg) Weight (kg) Simulated Plasma DEX Concentrations • Bottom line – 0.25 mcg/kg/hour without a bolus • Middle line – Bolus of 0.35 mcg/kg over ten min followed by 0.25 mcg/kg/hr • Top line - Bolus of 0.75 mcg/kg over ten min followed by 0.25 mcg/kg/hour Design and Conduct • Dose escalation study • Loading dose immediately followed by a continuous intravenous infusion (CIVI) • Dexmedetomidine infusion ≤ 24 hours Individual Predicted Plasma Concentration (pg/mL) • Final model: • CL = θCL * (WT/ 7.0)0.75 • Q = θQ * (WT/ 7.0)0.75 *(TBYP/58) θTBYP • V1 = θV1 • V2 = θV2* (WT/ 7.0)1 Methods B. B. A. Safety Monitoring • Cardiovascular events • 3 subjects with increased cardiac ischemia possibly related to study drug not clinically significant (Dose 1, n = 2; Dose 3 n = 1) • 1 subject developed intermittent accelerated junctional rhythm possibly related to study drug not clinically significant (Dose 2) • 1 subject developed intermittent complete heart block with bradycardia possibly related to study drug resulting in discontinuation of infusion (Dose 2) • 1 subject in Dose 3 developed oversedation and hypopnea requiring discontinuation of infusion • No evidence of elevated transaminases, ocular dryness or clinically significant adrenal suppression • Drop-outs • 1 subject experienced hypotension with ongoing post-operative bleeding during administration of bolus dose without initiation of infusion • 1 subject was removed from study due to leakage of peripheral IV catheter Minutes Validated liquid chromatography & tandem mass spectrometry assay Base Model • NONMEM ADVAN 3, TRANS 4 first order conditional estimation (FOCE) with interaction • Two-compartment disposition model Clearance (CL, mL/min), inter-compartmental clearance (Q, mL/min) volume of central compartment (V1, L), volume of peripheral compartment (V2, L). • Exponential error model for inter-individual variability • Additive and proportional error model for random residual variability Covariate analysis • Covariate analysis included age, weight, total cardiopulmonary bypass time, cross clamp time, and circulatory arrest time as continuous variables and ventricular physiology (single or two ventricles) as a categorical variable Simulations • Final model was used to perform 500 simulations for an infant with a weight of 7.0 kg who received 58 minutes of cardiopulmonary bypass with a fixed rate infusion of 0.25 mcg/kg/hour: • No bolus dose • 0.35 mcg/kg bolus • 0.75 mcg/kg bolus • Median plasma concentrations were plotted against time to assess the impact of the bolus dose on the time to steady state concentration 1Hospira, Precedex Product Label 2004 2Petroz GC, et al. Anesthesiology 2006. 105:1098–1110 Conclusions Individual Predicted vs. Observed Concentration Population Predicted vs. Observed Concentration • Dexmedetomidine appears to be safe in infants with congenital heart disease following open heart surgery • The were no serious adverse events attributed to study drug • In infants following open heart surgery, dexmedetomidineclearance and volume of distribution is higher than reported values in older children • Single versus two-ventricle physiology did not impact dexmedetomidine pharmacokinetics • Without an appropriate loading dose, time to steady state concentration is approximately 6 hours after the initiation of a continuous infusion • Simulations suggest that a ratio of the bolus dose to continuous infusion rate of 3:1 is required to achieve steady state concentrations rapidly Individual Predicted Plasma Concentration (pg/mL) Population Predicted Plasma Concentration (pg/mL) Acknowledgements Observed Plasma Concentrations (pg/mL) Observed Plasma Concentrations (pg/mL)