Download
1 / 14
140 likes | 180 Vues
Learn about different types of motor neuron diseases, their clinical findings, investigation methods, and treatment options. Dive into the complexities of Motor Neuron Disease in Adults and Children. Discover the classification, clinical symptoms, differential diagnoses, typical investigations, and management strategies. Gain insights into the debilitating effects of degenerative diseases of the nervous system. Stay informed and find support for coping with these challenging conditions.

E N D
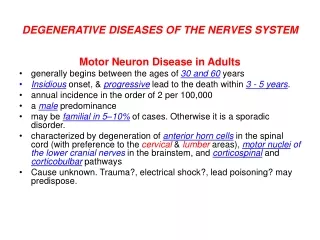
DEGENERATIVE DISEASES OF THE NERVES SYSTEM Motor Neuron Disease in Adults • generally begins between the ages of 30 and 60 years • Insidious onset, & progressive lead to the death within 3 - 5 years. • annual incidence in the order of 2 per 100,000 • a male predominance • may be familial in 5–10% of cases. Otherwise it is a sporadic disorder. • characterized by degeneration of anterior horn cells in the spinal cord (with preference to the cervical&lumberareas), motor nuclei of the lower cranial nerves in the brainstem, and corticospinal and corticobulbar pathways • Cause unknown. Trauma?, electrical shock?, lead poisoning? may predispose.
Classification: 5 types: • Progressive Bulbar Palsy: Bilateral involvement of motor nuclei of lower 4 cranial nerves in the brain stem, • Pseudobulbar Palsy: Bilateral involvement of corticobulbar pathways of 9th , 10th , 12th cranial nerves, • Progressive Spinal Muscular Atrophy: Lower motor neuron signs in the limbs, caused by anterior horn cells degeneration in the spinal cord, • Primary Lateral Sclerosis: Rare. Pure upper motor neuron signs are found in the limbs due to pure corticospinal tracts involvement, • Amyotrophic Lateral Sclerosis (most common form): A mixed upper and lower motor neuron deficit is found in the limbs. There may also be bulbar involvement of the upper or lower motor neuron type.
Clinical Findings: In 20% of patients with amyotrophic lateral sclerosis, the initial disturbances related to weakness of bulbar muscles (Bulbar / Pseudobulbar Palsy). In 40% the initial symptoms due to involvement of upper limbs. In other 40% the disease involve lower limbs initially. Bulbar involvement is generally characterized symptomatically by difficulty in swallowing, chewing, coughing, breathing, and speaking (dysarthria) Limbs involvement is characterized symptomatically by easy fatigability, weakness, stiffness, twitching (fasciculation), wasting, and muscle cramps (the earliest complain), and there may be vague sensory complaints and weight loss Involvement of the limbs is asymmetrical, but ultimately it will become symmetrical. Examination reveals upper, or lower, or combination of upper+lower motor neuron signs e.g: (fasciculation, m. atrophy, spasticity, upgoing planters) depending upon the type of the disease. There is no sensory signs No involvement of extra-ocular muscles or sphincters
Differential diagnosis: • Cervical spondylosis • Cervical cord compression by tumor • Foremen magnum tumor • Multifocal motor neuropathy • Chronic lead poisoning Investigation: • MRI of cervical spine & foramen magnum to exclude tumors • EMG (show denervations) & NCS (normal) • C.P.K enzyme is normal or mildly elevated • Muscle biopsy (show denervations) Definitive diagnosis requires the presence of combined upper and lower motor neuron signs in the bulbar region+ at least two spinal regions (cervical, thoracic, or lumbosacral), or in three spinal regions. Treatment: no specific treatment available. Riluzole 100 mg/d in 2 divided doses slightly slow the progression of disease. It prolong life of patient for 2 – 3 months only no more. It act by reduce excitotoxicity by diminishing glutamate release. Otherwise the treatment is merely symptomatic. NG tube needed if patient develop sever dysphagia. Tracheotomy & mechanical ventilation needed when sever respiratory difficulties developed.
Motor Neuron Disease in Children • a group of genetically determined disorders affecting spinal motor and cranial motor neurons, characterized by proximal and distal wasting, fasciculation and weakness of muscles. Involvement is usually symmetrical & affect proximal muscles more than distal ones. Treatment just symptomatic. 1) Infantile Spinal Muscular Atrophy (Werdnig-Hoffmann Disease or SMA-I): autosomal recessive. manifests itself within the first 3 months of life. the infant is floppy (hypotonic) difficulty with sucking, swallowing, or ventilation (early bulbar involvement) the tendon reflexes are normal or depressed the plantar responses may be absent It is a rapidly progressive disease leading to death from respiratory complications by about 3 years of age
2) Intermediate Spinal Muscular Atrophy (Chronic Werdnig-Hoffmann Disease or SMA-II): autosomal recessive begins in the 2nd half of the first year wasting and weakness of the extremities bulbar weakness occurs less commonly progresses slowly & its course is more benign many patients survive into adulthood 3) Juvenile Spinal Muscular Atrophy (Kugelberg-Welander Disease or SMA-III): develops in childhood or early adolescence, on either a hereditary or sporadic basis. The usual mode of inheritance is autosomal recessive. It particularly tends to affect the proximal limb muscles generally little involvement of the bulbar musculature. It follows a gradually progressive course leading to disability in early adult life
Syringomyelia • Is cavitation of the spinal cord. • 2 types: 1) Communicating syringomyelia—with communication between the central canal of the cord and the cavity—is a hydrodynamic disorder of the CSF pathways. It associated with: • Arnold-Chiari malformation (lead to hydrocephalus, cerebellar ataxia, pyramidal and sensory deficits in the limbs, and abnormalities of the lower cranial nerves, alone or in any combination) • Chronic arachnoiditis of the basal cisterns 2) Non-communicating syringomyelia, there is cystic dilation of the cord, which is not in communication with the CSF pathways It caused by: • trauma (start several years – rarely a few months- after the spinal injury) • intramedullary spinal tumors • spinal arachnoiditis
Clinical features:(asymmetrical) • a dissociated sensory lossat the level of the lesion; impaired pinprick and temperature appreciation, but preserved light touch sensation (involvement of spino-thalamic tracts). • Cavitation commonly occurs in the cervical region; this can cause a capelike distribution of sensory loss over one or both shoulders, diffuse pain in the neck, and radicular pain in the arms • Sensory impairment lead to trophic changes in upper limbs: painless skin ulcers, scars, edema, hyperhidrosis, neuropathic joints, resorption of the terminal phalanges. • Weakness and wasting of muscles occur at the level of the lesion because of the involvement of the anterior horns of the cord. • The tendon reflexes may be depressed at the level of the lesion • A pyramidal deficit and sphincter disturbances sometimes occur below the level of the lesion because of involvement of the corticospinal pathways & autonomic tracts respectively. • involvement of the T1 segment frequently leads to ipsilateral Horner syndrome • Scoliosis, pes cavus.
Some time the cavitation extend upward into the lower part of brain stem (medulla oblongata). For this condition the term “syringobulbia” will be applied. • In syringobulbia there will be additional features of bulbar palsy (absent gag & palatal reflexes, dysarthria −nasal speech−, dysphagia, nasal regurgitation, atrophied fasciculated tongue)
Investigation: MRI, or CT scanning (including the foremenmagnum region to show if there is associated Chiari malformation) confirms the diagnosis. They will show cavitation inside the cord that not take enhancement; a feature differentiate it from intramedullary spinal tumors Treatment: is surgical. Prognosis:is bad because surgical treatment is disappointing, i.e. condition frequently reoccur after correct surgery!!
MRI show syringomyelia in 2 patients (Left: T1 weighted of a case, Right: T2 weighted of other case)
Familial Spastic Paraplegia • In its pure form, FSP is usually transmitted as an autosomal trait. • Most adult-onset cases are dominantly inherited • It arises in the third or fourth decade • there is degeneration of the corticospinal tracts • There is progressive spastic paraparesis beginning in the distal lower extremities eventually lead to paraplegia • Late in the illness there may be urinary urgency and incontinence and sometimes fecal incontinence; • sexual function tends to be preserved • Treatment is symptomatic.
Multiple systems atrophy (MSA) • Sporadic disease • Usually affect middle-aged and elderly • Parkinsonism, often without tremor, are combined with varying degrees of autonomic failure, cerebellar involvement and pyramidal tract dysfunction • Combination of parkinsonism with autonomic failure was called the Shy-Drager syndrome • Degeneration is more widespread than Parkinson’s disease • There is disappointing response to levodopa and other anti-parkinsonian drugs • Falls are much more common than in idiopathic Parkinson's disease. As a result from this: • life expectancy, is considerably reduced. • Treatment is just symptomatic