Download
1 / 16
160 likes | 374 Vues
Background. Reproductive health essential and integral component of women's overall health and well-beingTypically defined as contraception, STD and other screening, maternity care, abortion, and infertilityUse of services affected by a broad range of federal and state policies and financing sy

E N D
1. Reproductive Health Care for Women: Coverage, Access, and Financing Hello. I�m Usha Ranji, Senior Policy Analyst in Women�s Health Policy at the Kaiser Family Foundation.
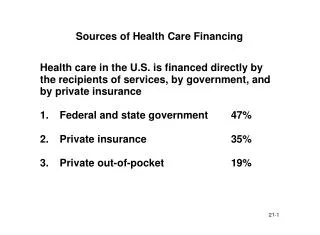
Reproductive health care is central to women�s overall health and physical, social, and psychological well-being. In the U.S., how women use reproductive care is in large part shaped by the public and private sector policies that affect women�s health insurance coverage as well as the availability and affordability of those services.
In this tutorial, I�ll discuss some of the key health policies of importance to women that govern their coverage and access to reproductive health services as well as the financing of these services for women in their reproductive years. Hello. I�m Usha Ranji, Senior Policy Analyst in Women�s Health Policy at the Kaiser Family Foundation.
Reproductive health care is central to women�s overall health and physical, social, and psychological well-being. In the U.S., how women use reproductive care is in large part shaped by the public and private sector policies that affect women�s health insurance coverage as well as the availability and affordability of those services.
In this tutorial, I�ll discuss some of the key health policies of importance to women that govern their coverage and access to reproductive health services as well as the financing of these services for women in their reproductive years.
2. Background Reproductive health essential and integral component of women�s overall health and well-being
Typically defined as contraception, STD and other screening, maternity care, abortion, and infertility
Use of services affected by a broad range of federal and state policies and financing systems
Private insurance also shapes access to certain reproductive services for women.
Over the course of their reproductive years, women need a broad range of preventive and treatment services such as contraception, screening for sexually transmitted diseases, prenatal and maternity care, abortion, infertility services.
These services are typically defined as reproductive care.
Women�s ability to obtain the full range of reproductive services is shaped by several factors. These include state and federal public policies related to financing and delivery of care and whether they have insurance coverage or not.
Over the course of their reproductive years, women need a broad range of preventive and treatment services such as contraception, screening for sexually transmitted diseases, prenatal and maternity care, abortion, infertility services.
These services are typically defined as reproductive care.
Women�s ability to obtain the full range of reproductive services is shaped by several factors. These include state and federal public policies related to financing and delivery of care and whether they have insurance coverage or not.
3. Prevention Women in their reproductive years typically need a number of preventive services. These include contraception, Pap smears and breast exams, as well as screening and protection from sexually transmitted infections, such as HPV, chlamydia, and HIV/AIDS. Women in their reproductive years typically need a number of preventive services. These include contraception, Pap smears and breast exams, as well as screening and protection from sexually transmitted infections, such as HPV, chlamydia, and HIV/AIDS.
4. Family planning or contraceptive services allow women to prevent unintended pregnancies and plan and space their childbearing if they choose to have children. It has been estimated that a woman who plans to have two children in her lifetime may spend up to 30 years in need of some form of contraception.
Having insurance coverage for contraception makes it more affordable and for some women facilitates access. Two-thirds of women of reproductive age are covered by employer-sponsored plans. In the past, many plans did not cover contraceptives in their benefit packages meaning that women had to pay for contraceptives out-of-pocket .
While there is no federal law requiring that employer-based plans cover contraceptives, several states have passed laws that require employer-sponsored plans to provide insurance coverage for contraceptives. These laws vary, though, and several exempt insurers or employers from the requirement, if they have religious or moral objections to contraception. Furthermore, these state insurance laws do not apply to self-funded plans, which cover about half of all workers.
These laws have been reinforced by several federal court rulings that have stated that employers must cover contraceptives to the same extent they cover other prescription drugs, devices, and preventive services.
Employer-sponsored coverage of contraceptives has improved over the last several years. In 2004 89% of insured workers had coverage for oral contraceptives. While this represents significant growth in just a few years, this figure still lags behind the 100% coverage for other prescription drugs.
Family planning or contraceptive services allow women to prevent unintended pregnancies and plan and space their childbearing if they choose to have children. It has been estimated that a woman who plans to have two children in her lifetime may spend up to 30 years in need of some form of contraception.
Having insurance coverage for contraception makes it more affordable and for some women facilitates access. Two-thirds of women of reproductive age are covered by employer-sponsored plans. In the past, many plans did not cover contraceptives in their benefit packages meaning that women had to pay for contraceptives out-of-pocket .
While there is no federal law requiring that employer-based plans cover contraceptives, several states have passed laws that require employer-sponsored plans to provide insurance coverage for contraceptives. These laws vary, though, and several exempt insurers or employers from the requirement, if they have religious or moral objections to contraception. Furthermore, these state insurance laws do not apply to self-funded plans, which cover about half of all workers.
These laws have been reinforced by several federal court rulings that have stated that employers must cover contraceptives to the same extent they cover other prescription drugs, devices, and preventive services.
Employer-sponsored coverage of contraceptives has improved over the last several years. In 2004 89% of insured workers had coverage for oral contraceptives. While this represents significant growth in just a few years, this figure still lags behind the 100% coverage for other prescription drugs.
5. Medicaid and Family Planning There are several public sector programs that finance family planning services for low-income women. The Medicaid program is a major payer for family planning services. Medicaid is the federal-state health insurance program for the nation�s low-income families. Family planning has a special status in Medicaid, because the federal government pays a larger share of the costs for family planning services than they do for other health care.
Nearly 6 million women of reproductive age are covered by Medicaid and rely on it for their health care needs, including reproductive health services. Medicaid accounts for 61% of all publicly-financed family planning services.
Most states typically provide coverage for oral contraceptives, gynecological exams, condoms, and STD testing. In recent years, several states have also extended Medicaid eligibility for family planning services only to low-income women who would not otherwise qualify for the full range of Medicaid benefits.
Currently, federal and state policymakers are debating the Medicaid program�s future and considering budget cuts because of fiscal shortfalls at the state and federal levels. Depending on the outcome of these debates, these changes could have an impact on family planning services for women on Medicaid.There are several public sector programs that finance family planning services for low-income women. The Medicaid program is a major payer for family planning services. Medicaid is the federal-state health insurance program for the nation�s low-income families. Family planning has a special status in Medicaid, because the federal government pays a larger share of the costs for family planning services than they do for other health care.
Nearly 6 million women of reproductive age are covered by Medicaid and rely on it for their health care needs, including reproductive health services. Medicaid accounts for 61% of all publicly-financed family planning services.
Most states typically provide coverage for oral contraceptives, gynecological exams, condoms, and STD testing. In recent years, several states have also extended Medicaid eligibility for family planning services only to low-income women who would not otherwise qualify for the full range of Medicaid benefits.
Currently, federal and state policymakers are debating the Medicaid program�s future and considering budget cuts because of fiscal shortfalls at the state and federal levels. Depending on the outcome of these debates, these changes could have an impact on family planning services for women on Medicaid.
6. Title X Publicly-financed network of clinics and providers for family planning services
Serves ~ 5 million low-income women annually
Funding levels have not kept up with inflation and demand Another important public program in the financing of reproductive health care is the Federal Title X program. This program is administered by the federal Department of Health and Human Services� Office of Population Affairs, the national agency charged with oversight of several important reproductive health programs and policies.
Title X consists of a network of family planning clinics that serves approximatley 5 million low-income women annually. Many of these women do not qualify for the Medicaid program and are uninsured, and without the program would not likely have access to or be able to afford the reproductive health services provided at these clinics. Services covered under Title X include contraception, STD testing, and referrals to prenatal care.
The Title X program, though has been under growing financial strain in recent years. The number of women eligible for the program has grown as have the costs of contraceptives and other services. The program receives an annual funding level appropriation, determined by Congress and the President. As you can see in this chart, while the funding level has increased over several years, when inflation is taken into account, the buying power of the program has actually had a decreased over time.
Another important public program in the financing of reproductive health care is the Federal Title X program. This program is administered by the federal Department of Health and Human Services� Office of Population Affairs, the national agency charged with oversight of several important reproductive health programs and policies.
Title X consists of a network of family planning clinics that serves approximatley 5 million low-income women annually. Many of these women do not qualify for the Medicaid program and are uninsured, and without the program would not likely have access to or be able to afford the reproductive health services provided at these clinics. Services covered under Title X include contraception, STD testing, and referrals to prenatal care.
The Title X program, though has been under growing financial strain in recent years. The number of women eligible for the program has grown as have the costs of contraceptives and other services. The program receives an annual funding level appropriation, determined by Congress and the President. As you can see in this chart, while the funding level has increased over several years, when inflation is taken into account, the buying power of the program has actually had a decreased over time.
7. Access to Emergency Contraception Over the last several years, there has been growing attention to emergency contraception, sometimes referred to as the �morning-after� pill. Emergency contraception is a back-up method of birth control. It is a pre-packaged form of high dose birth control pills that can be taken after unprotected sex to prevent a pregnancy. If used within a few days, it is highly effective in preventing pregnancy, and if a woman is already pregnant, EC does not affect the pregnancy.
In recent years, there has been rising awareness about the availability of EC among women, but still many do not know about this option. Approximately one-third of women of reproductive age report that they did not know that there is something that a woman can do to prevent pregnancy after intercourse.
On the policy front, the manufacturer of Plan B, the major form of EC pills, has applied to the Food and Drug Administration for approval to make EC available over-the-counter rather than with a doctor�s prescription as currently required. This application has been under review for several years and a final decision from the FDA is pending.
At the state level, there has also been interest in expanding access to EC. Seven states allow pharmacists to dispense EC without a doctor�s prescription and eight states require hospital emergency rooms to offer or provide a referral for EC to survivors of sexual assault.
Despite these efforts to enhance access to emergency contraception, there have been reports of pharmacists who have refused to dispense EC because of moral or religious objections to the drug. Some states have enacted measures to help assure that women can obtain EC when they go to a pharmacy. Over the last several years, there has been growing attention to emergency contraception, sometimes referred to as the �morning-after� pill. Emergency contraception is a back-up method of birth control. It is a pre-packaged form of high dose birth control pills that can be taken after unprotected sex to prevent a pregnancy. If used within a few days, it is highly effective in preventing pregnancy, and if a woman is already pregnant, EC does not affect the pregnancy.
In recent years, there has been rising awareness about the availability of EC among women, but still many do not know about this option. Approximately one-third of women of reproductive age report that they did not know that there is something that a woman can do to prevent pregnancy after intercourse.
On the policy front, the manufacturer of Plan B, the major form of EC pills, has applied to the Food and Drug Administration for approval to make EC available over-the-counter rather than with a doctor�s prescription as currently required. This application has been under review for several years and a final decision from the FDA is pending.
At the state level, there has also been interest in expanding access to EC. Seven states allow pharmacists to dispense EC without a doctor�s prescription and eight states require hospital emergency rooms to offer or provide a referral for EC to survivors of sexual assault.
Despite these efforts to enhance access to emergency contraception, there have been reports of pharmacists who have refused to dispense EC because of moral or religious objections to the drug. Some states have enacted measures to help assure that women can obtain EC when they go to a pharmacy.
8. Access for Young Women Major policy proposals centered on access to information, preventive, and treatment services, including contraception and abortion
Declining rates of teen pregnancy but STDs remain public health challenge
Push for greater parental involvement (consent/notification laws for reproductive care)
Sex education � expansion of abstinence-only programs; debates over impact on youth One area of considerable policy attention has been about reproductive health services for young women, particularly the extent to which teens should be allowed access without parental consent or notification to family planning and treatment services, particularly contraception and abortion.
While rates of teenage pregnancy have been on the decline for the past two decades, it is still a problem in many communities, and many young women are still at risk for sexually transmitted diseases. On a policy level, there has been a push for increased parental involvement, including the passage of several state parental consent and notification laws in order for minors to obtain abortions. Legislation has also been introduced that would require parental consent for contraception, but this legislation has not passed.
Over the past several years, there has also been a shift in sex education policy with expansion in federal funding for and teaching of abstinence-only programs, which do not include instruction about contraceptive options in school curricula. This has generated considerable debate and ongoing research over the impact of these programs.One area of considerable policy attention has been about reproductive health services for young women, particularly the extent to which teens should be allowed access without parental consent or notification to family planning and treatment services, particularly contraception and abortion.
While rates of teenage pregnancy have been on the decline for the past two decades, it is still a problem in many communities, and many young women are still at risk for sexually transmitted diseases. On a policy level, there has been a push for increased parental involvement, including the passage of several state parental consent and notification laws in order for minors to obtain abortions. Legislation has also been introduced that would require parental consent for contraception, but this legislation has not passed.
Over the past several years, there has also been a shift in sex education policy with expansion in federal funding for and teaching of abstinence-only programs, which do not include instruction about contraceptive options in school curricula. This has generated considerable debate and ongoing research over the impact of these programs.
9. Women as a Proportion of Newly Reported AIDS Cases, 1986-2002 Proportion more than tripled since beginning of epidemic
Women of color, particularly African Americans, disproportionately affected
Heavy concentration in Southern region
Young women at particular risk One alarming trend in the field of reproductive health is the growing representation of women in the HIV/AIDS epidemic in the U.S. Over the course of the epidemic�s history, heterosexual contact has become the predominant mode of transmission of HIV. While the majority of cases of HIV and AIDS are still among men, women now comprise one-fourth of new AIDS cases, a proportion that has more than tripled since the early years of the epidemic. HIV/AIDS has disproportionately affected women of color, particularly African American women, who make up the largest share of new infections among women. The epidemic is heavily concentrated in the Southern region of the country. And young women are particularly vulnerable and increasingly represent the face of this epidemic.One alarming trend in the field of reproductive health is the growing representation of women in the HIV/AIDS epidemic in the U.S. Over the course of the epidemic�s history, heterosexual contact has become the predominant mode of transmission of HIV. While the majority of cases of HIV and AIDS are still among men, women now comprise one-fourth of new AIDS cases, a proportion that has more than tripled since the early years of the epidemic. HIV/AIDS has disproportionately affected women of color, particularly African American women, who make up the largest share of new infections among women. The epidemic is heavily concentrated in the Southern region of the country. And young women are particularly vulnerable and increasingly represent the face of this epidemic.
10. Pregnancy and Maternity Care Pregnancy is a defining event of the reproductive years for many women. Pregnancy and related maternity care have also been the source of a number of public policy initiatives.Pregnancy is a defining event of the reproductive years for many women. Pregnancy and related maternity care have also been the source of a number of public policy initiatives.
11. Pregnancy In the U.S., there are over 6 million pregnancies annually. Although use of contraception has been rising for several years, as you can see from this chart, approximately half of all pregnancies are still unintended.
In the U.S., there are over 6 million pregnancies annually. Although use of contraception has been rising for several years, as you can see from this chart, approximately half of all pregnancies are still unintended.
12. Major Federal Pregnancy-Related Legislation Pregnancy Discrimination Act of 1978
Gradual expansion in employer-based health benefits � most workers covered for prenatal care, contraceptives, annual Ob/Gyn visit, maternity leave
Family and Medical Leave Act of 1993
Workplace protections for unpaid maternity leave and time off to care for family members
First paid family leave law passed in CA in 2002
Newborns' and Mothers' Protection Act of 1996
Ban �drive thru� deliveries
Hospital stay for childbirth may not be restricted to less than 48 hours following a vaginal birth or 96 hours for cesarean �
Maternity care has been the focal point of some major pieces of federal legislation. One of the first was the Pregnancy Discrimination Act of 1978, which helped protect women�s job security by making it illegal to discriminate against women in the workplace because of a pregnancy. This includes protections in hiring practices, career advancement, as well as return to work after maternity leave. This law has resulted in large-scale expansion in health benefits related to pregnancy, with most workers covered for prenatal care, rising numbers covered for contraception, and an annual OB visit.
Another landmark law was the Family and Medical Leave Act, which allows women to take time off from work after having a baby or to care for an ailing family member, and still keep their jobs. While this law guarantees protections for unpaid leave, only the state of CA recently provided paid time off for maternity or other family leave.
And in response to concerns about so-called �drive thru deliveries� when many women were only covered for a 24 hour hospital stay following a normal delivery, Congress passed the Newborns and Mothers Protection Act. This law mandated that the hospital stays for deliveries could not be restricted to fewer than 48 hours and came on the heels of several similar state initiatives.
Maternity care has been the focal point of some major pieces of federal legislation. One of the first was the Pregnancy Discrimination Act of 1978, which helped protect women�s job security by making it illegal to discriminate against women in the workplace because of a pregnancy. This includes protections in hiring practices, career advancement, as well as return to work after maternity leave. This law has resulted in large-scale expansion in health benefits related to pregnancy, with most workers covered for prenatal care, rising numbers covered for contraception, and an annual OB visit.
Another landmark law was the Family and Medical Leave Act, which allows women to take time off from work after having a baby or to care for an ailing family member, and still keep their jobs. While this law guarantees protections for unpaid leave, only the state of CA recently provided paid time off for maternity or other family leave.
And in response to concerns about so-called �drive thru deliveries� when many women were only covered for a 24 hour hospital stay following a normal delivery, Congress passed the Newborns and Mothers Protection Act. This law mandated that the hospital stays for deliveries could not be restricted to fewer than 48 hours and came on the heels of several similar state initiatives.
13. Medicaid and Maternity Care In response to high rates of infant mortality and low birthweight, state and federal policymakers began a series of eligibility expansions for pregnant women to enroll in Medicaid to improve access to prenatal care, starting in the late 1980s. Medicaid covers a broad range of pregnancy-related care, such as prenatal care, hospitalization, and post-partum care for mothers. All states must extend coverage to pregnant women living below 133% of the federal poverty level, or about $21,000 for a family of three. As you can see, these eligibility levels are far higher than they are for other adults. Many states, however, go beyond this minimum threshold and have also adopted policies to ease enrollment for pregnant women. Today, Medicaid covers nearly 40% of births throughout the country, and in some states, it is over half of all births.
All infants born to mothers on Medicaid are guaranteed coverage for their first year of life. Their mothers, though, are guaranteed coverage for 60 days post-partum, and lose their coverage unless they qualify for Medicaid under a different eligibility pathway. In response to high rates of infant mortality and low birthweight, state and federal policymakers began a series of eligibility expansions for pregnant women to enroll in Medicaid to improve access to prenatal care, starting in the late 1980s. Medicaid covers a broad range of pregnancy-related care, such as prenatal care, hospitalization, and post-partum care for mothers. All states must extend coverage to pregnant women living below 133% of the federal poverty level, or about $21,000 for a family of three. As you can see, these eligibility levels are far higher than they are for other adults. Many states, however, go beyond this minimum threshold and have also adopted policies to ease enrollment for pregnant women. Today, Medicaid covers nearly 40% of births throughout the country, and in some states, it is over half of all births.
All infants born to mothers on Medicaid are guaranteed coverage for their first year of life. Their mothers, though, are guaranteed coverage for 60 days post-partum, and lose their coverage unless they qualify for Medicaid under a different eligibility pathway.
14. Trends in Abortion Half of unintended pregnancies end in abortion
Overall rate declining, but not among low-income women
Majority occur within first trimester
74% are self-pay As I said earlier, half of all pregnancies are unintended and half of these end in abortion. In 2002, nearly 1.3 million pregnancies were terminated by abortion. In the U.S., among women overall, abortions have been on the decline. A number of possible factors may account for this, including more effective use of contraception, greater acceptance of childbearing outside of marriage, and increased restrictions on access to abortion. However, among certain sub-groups of women, notably low-income women, the rate of abortions has been on the rise.
Most abortions occur within the first trimester of pregnancy. Three-quarters of abortion are paid for out-of-pocket. This may be due to the fact that Medicaid coverage for abortions is very limited, and that individuals with private insurance either may not know that they have coverage or choose not to use their insurance because of privacy concerns.As I said earlier, half of all pregnancies are unintended and half of these end in abortion. In 2002, nearly 1.3 million pregnancies were terminated by abortion. In the U.S., among women overall, abortions have been on the decline. A number of possible factors may account for this, including more effective use of contraception, greater acceptance of childbearing outside of marriage, and increased restrictions on access to abortion. However, among certain sub-groups of women, notably low-income women, the rate of abortions has been on the rise.
Most abortions occur within the first trimester of pregnancy. Three-quarters of abortion are paid for out-of-pocket. This may be due to the fact that Medicaid coverage for abortions is very limited, and that individuals with private insurance either may not know that they have coverage or choose not to use their insurance because of privacy concerns.
15. Access and Financing Abortion Services
Federal Policy
Hyde Amendment bans Federal financing of abortions except in cases of rape, incest, or to save the life of the woman
Medicaid
Women in military
�Partial birth� abortion ban � ruled unconstitutional, passed by Congress and signed by President
State Policy
�Partial birth� bans
Waiting periods
Provider/Facility Regulations
Parental consent/notification for minors,
Health care provider refusal clauses
Abortion is highly regulated at both the federal and state levels. At the federal level, the Hyde Amendment limits federal financing for abortions to cases of rape, incest, or a threat to the life of the woman. This means that no federal dollars can be used for other cases. This has a large impact on Medicaid. States can, however, opt to use their own dollars to pay for abortions in other, limited cases. Currently, 17 states do so. The Hyde Amendment also affects access for women in the military, who cannot obtain abortions using federal funds.
The federal ban on certain types of abortion procedures, known as the partial birth abortion ban was signed by the President in 2003, but its constitutionality has been under review in the courts because of its potential impact on medical practice and access to abortion services.
At the state level, several different policies have been enacted that affect women�s access to abortion. These include state-level partial birth bans in 31 states, as well as a mix of mandatory waiting periods, increased regulations for abortion clinics, parental consent and notification laws for minors, and refusal or �conscience� clauses which allow health care providers, employers, and insurance plans to refuse coverage, referral, or provision of abortion services due to moral or ethical objections.Abortion is highly regulated at both the federal and state levels. At the federal level, the Hyde Amendment limits federal financing for abortions to cases of rape, incest, or a threat to the life of the woman. This means that no federal dollars can be used for other cases. This has a large impact on Medicaid. States can, however, opt to use their own dollars to pay for abortions in other, limited cases. Currently, 17 states do so. The Hyde Amendment also affects access for women in the military, who cannot obtain abortions using federal funds.
The federal ban on certain types of abortion procedures, known as the partial birth abortion ban was signed by the President in 2003, but its constitutionality has been under review in the courts because of its potential impact on medical practice and access to abortion services.
At the state level, several different policies have been enacted that affect women�s access to abortion. These include state-level partial birth bans in 31 states, as well as a mix of mandatory waiting periods, increased regulations for abortion clinics, parental consent and notification laws for minors, and refusal or �conscience� clauses which allow health care providers, employers, and insurance plans to refuse coverage, referral, or provision of abortion services due to moral or ethical objections.
16. Infertility Broader range of treatments now available
Use of ARTs estimated to have nearly doubled between 1996 and 2002
Costs $12,000 on average per IVF cycle
Relatively limited insurance coverage; 15 states mandate at least limited coverage for diagnosis and treatment Infertility affects millions of women in the U.S. Over the years, several different forms of medical treatments have emerged to aid with conception, ranging from prescription medications to surgical interventions to in vitro fertilization. The use of ARTs, which include in vitro fertilization, has nearly doubled in the last several years as you can see in this chart.
However, the growth of ARTs has raised several important issues about health care costs and coverage. Many of these procedures are very expensive. For example, the average cost of an in vitro fertilization is approximately $12,000 per cycle. Currently, there is relatively little insurance coverage for these procedures. This makes some ARTs available only to those who can afford to pay for the services out-of-pocket. 15 states have some sort of mandate for insurers, ranging from coverage for diagnosis and treatment to selling coverage for infertility. Several of these states also allow insurers and employers to opt out if they hold religious or moral objections to infertility treatment.
Infertility affects millions of women in the U.S. Over the years, several different forms of medical treatments have emerged to aid with conception, ranging from prescription medications to surgical interventions to in vitro fertilization. The use of ARTs, which include in vitro fertilization, has nearly doubled in the last several years as you can see in this chart.
However, the growth of ARTs has raised several important issues about health care costs and coverage. Many of these procedures are very expensive. For example, the average cost of an in vitro fertilization is approximately $12,000 per cycle. Currently, there is relatively little insurance coverage for these procedures. This makes some ARTs available only to those who can afford to pay for the services out-of-pocket. 15 states have some sort of mandate for insurers, ranging from coverage for diagnosis and treatment to selling coverage for infertility. Several of these states also allow insurers and employers to opt out if they hold religious or moral objections to infertility treatment.
17. Conclusions Range of reproductive health services has expanded tremendously
Access is central to women�s overall health and well-being
Federal and state policies wield significant influence on reproductive health
Likely to continue to be at center of several policy debates
So in conclusion, reproductive health care is central to women�s health and well-being. Over the last several decades, there have been major advances in the field of reproductive health care that now allow women more options to prevent unintended pregnancies, to have healthy pregnancies and families, to screen for and treat STDs and HIV, and to address infertility.
On a policy level, there is a wide array of private and public programs that finance reproductive health care in the U.S., and there have been several efforts at the federal and state levels to broaden women�s access to services, including mandates for private insurance coverage, a greater role for the Medicaid program, and enactment of legislation to protect the rights of pregnant women. At the same time, there is continuing disagreement on some key elements of reproductive health policy, such as abortion, sex education, and the provision of contraception to teens. As the field of women�s health and reproductive health continues to evolve, we will likely be faced with these and yet unknown policy debates. So in conclusion, reproductive health care is central to women�s health and well-being. Over the last several decades, there have been major advances in the field of reproductive health care that now allow women more options to prevent unintended pregnancies, to have healthy pregnancies and families, to screen for and treat STDs and HIV, and to address infertility.
On a policy level, there is a wide array of private and public programs that finance reproductive health care in the U.S., and there have been several efforts at the federal and state levels to broaden women�s access to services, including mandates for private insurance coverage, a greater role for the Medicaid program, and enactment of legislation to protect the rights of pregnant women. At the same time, there is continuing disagreement on some key elements of reproductive health policy, such as abortion, sex education, and the provision of contraception to teens. As the field of women�s health and reproductive health continues to evolve, we will likely be faced with these and yet unknown policy debates.