Download
1 / 29
300 likes | 684 Vues
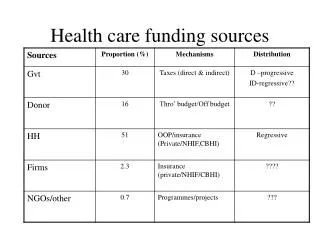
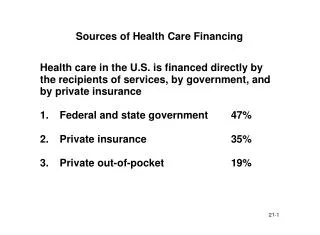
Sources of Health Care Financing. Health care in the U.S. is financed directly by the recipients of services, by government, and by private insurance 1. Federal and state government 47% 2. Private insurance 35% 3. Private out-of-pocket 19%. Coverage by Social Insurance Programs.

E N D
Sources of Health Care Financing • Health care in the U.S. is financed directly by the recipients of services, by government, and by private insurance • 1. Federal and state government 47% • 2. Private insurance 35% • 3. Private out-of-pocket 19%
Coverage by Social Insurance Programs • 1. Workers compensation pays medical expenses for work-related injuries. • 2. Federal Government is a major source of health care financing under two programs: • Medicare for persons over age 65. • Medicaid, a needs-based program for the poor.
Private Medical Expense Insurers • 1. Commercial insurance companies • 2. Blue Cross and Blue Shield • 3. Capitating health care providers • 4. Self insurers • corporate employers • Multiple Employer Trusts • MEWAs • 5. Federal CHAMPUS program
Extent of Medical Expense Coverage • 1. Most individuals under 65 (slightly less than two-thirds) are covered as employees or dependents under employer-sponsored medical expense plans. • 2. Where employer-sponsored coverage is not available, individual coverage may be purchased. • 3. Approximately 85% of Americans under age 65 were covered by private medical expense insurance in 1998.
Traditional Medical Expense Insurance Plans • GROUP MEDICAL EXPENSE INSURANCE • 1. Less than 10 million persons (under 5% of population) are insured under individually purchased medical expense insurance. • 2. Overwhelming dominance of group approach is due to • lower cost of group insurance • favorable tax treatment of employer-provided health insurance
Traditional Medical Expense Insurance Fee-For-Service Plans • Historically, commercial insurers and Blue Cross/Blue Shield organizations have provided fee-for-service benefits. • 1. insured sought services from a provider. • 2. insurance would pay some or all of the providers charge, directly or by reimbursing the insured. • 3. provider and insured agreed on the level of care and the insurer paid the bill.
Managed Care Plans • 1. Many experts argued that the fee-for-service approach provided an incentive to overutilize health care. • 2. Trend in recent years is away from traditional indemnity fee-for-service plans toward programs with a more direct relationship between the provider and the insurer. • 3. Newer approach includes HMOs, PPOs, and point-of-service plans. • 4. These programs are often referred to as managed care plans.
Traditional Fee-For-ServiceMedical Expense Insurance Plans • 1. Hospital expense coverage • 2. Surgical expense • 3. Physician’s expense coverage • 4. Major medical coverage
Hospitalization Insurance • 1. Hospital service benefit contracts • 2. Hospital reimbursement contracts • 3. Indemnity (cash payment) contracts
Surgical and Physician’s Expense Contracts • 1. Surgical service plans • 2. Surgical expense reimbursement contracts • 3. Physician’s expense reimbursement insurance
Major Medical Insurance • 1. High maximum (or unlimited) • 2. Deductible • 3. Coinsurance or share-loss provision
Comprehensive Major Medical $1,000,000 maximum Insurer pays 100% of costs up to maximum $10,000 Coinsured Layer of Coverage Insured pays 20% of Costs Insurer pays 80% of costs $250 per person/$500 family Deductible
Illustrated Payment Under Major Medical • Amount of loss $20,000 • Less deductible 250 • ______ • 19,750 • Insured pays 20% of expenseover deductible up to $10,000 $2,000 • Insurer pays balance $17,750
The Health Insurance Market Today • Although about 1,200 insurers that offer health insurance for medical expenses, traditional insurance plans no longer dominate the insurance market. • Many employers now offer health care coverage under alternative mechanisms. • 1. Health Maintenance Organizations • 2. Preferred Provider Organizations • 3. Point-of-Service Plans
GENERAL NATURE OF HMOs • Provide a wide range of comprehensive health care services to members in return for a fixed periodic payment. • Sponsored by a group of physicians, hospital, employer, labor union, consumer group, insurance company, or Blue Cross/Blue Shield plans. • HMO provides for the financing of health care and also delivers that care.
Provider Sponsored Organizations • 1. Also sometimes called • Physician-Hospital Organizations (PHOs) • Integrated Delivery Systems (IDS’s) • 2. Similar to HMOs • PHO’s are paid a capitated fee • fee is divided among providers on a prenegotiated basis
Preferred Provider Organizations (PPO’s) • 1. Doctors or hospitals with whom employer or insurer contracts to provide medical services. • 2. Provider discounts services and sets up utilization control programs to control costs. • 3. Employees not required to use PPO, but if they go elsewhere they must pay more.
Point of Service Plans (POS) • 1. POS plans are the newest development in health insurance field. • 2. In one respect, POS plans operate like a PPO, since the employee retains right to use any provider but will pay a higher part of the cost for a provider outside network. • 3. At same time, POS is like an HMO, since care received through network is managed by primary care physician or “gatekeeper.” • 4. POS plans were created when HMOs allowed subscribers to use nonnetwork providers.
Cost Containment Provisions • In addition to managed care arrangements such as HMOs, PPOs, and POS plans, most traditional indemnity plans have adopted cost control provisions. • 1. Increased employee cost sharing • 2. Coordination of benefits • 3. Covering alternative sites of care • 4. Addressing utilization
Dental Expense Insurance • Written with a dollar reimbursement limit or on a service basis. • Coinsurance may require different cost-sharing in earlier years (e.g., 50% first year, 60% second year, 70% third year, 80% fourth year and 90% thereafter). • Coinsurance may also be structured to encourage or discourage utilization (100% for preventive care, 50% for orthodontics)
Prescription Drugs • Usually written on a group basis, as an adjunct to other coverage. • Reimbursement Basis Coverage • Generally a coinsurance or deductible. • Deductible per prescription or annual. • Service basis Coverage • Operates similar to the Blue Cross model. • Insurer payments directly to pharmacists. • Payment limited to the amount payable to a participating pharmacy.
Medicaid • Title XIX of the Social Security Act, known as Medicaid, is a federal-state program of medical assistance for needy persons that was enacted simultaneously with the Medicare program. • provides medical assistance to low income persons and certain needy persons who are not at the poverty level. • the federal government sets regulations and minimum standards. • federal share of cost is based on a formula tied to state per capita income and varied from 50% to 80% in 1998.
Medicaid Benefits • Medicaid benefits are quite comprehensive. • Benefits includes services traditionally included in a commercial group-health-insurance plan and some services, such as long-term care, that are not. • Mandatory benefits in all states include inpatient and outpatient hospital services, physician services, and home health care. • Optional services include outpatient prescription drugs, prosthetic devices and hearing aids, and dental services.
Taxes and Health Care Costs • 1. Cost of employer-provided group plans is deductible by employer and nontaxable to the employee. • 2. For the individual, • health insurance premiums receive no special tax treatment. • premiums are combined with other health care costs and deductible to extent total exceeds 7.5% of AGI.
Health Insurance for Self-Employed • TRA-86 authorized self-employed persons to deduct 25% of cost of health insurance. The 25% later increased to 30% and then 40%. • TRA-97 phases in 100% deductibility. • Fiscal Year% Deductible • 1998-99 45% • 2000-01 50% • 2002 60% • 2003-2005 80% • 2006 90% • 2007 100%
The Health Insurance Problem • Access to health care • High cost of health care
The Access Problem • 40 million Americans have no health insurance coverage • Another 70 million are underinsured • Over 85% of the population with private insurance obtain coverage through employment
High Cost of Health Care • 1. Medical care costs growing faster than the average cost of living • 2. Consuming an increasing share of GNP • 1950 4.4% of GNP • 1998 13.+% of GNP
Some Causes of High Cost of Health Care and Health Insurance • Aging population • Improved (high-cost) medical technology • Excessive capacity • Defensive medicine • Insurance-encouraged utilization • Cost-shifting from government funded plans • Mandated benefits