Download
1 / 13
180 likes | 568 Vues
An Investigation of the Therac-25 Accidents. Nancy G. Leveson Clark S. Turner IEEE, 1993 Presented by Jack Kustanowitz April 26, 2005 University of Maryland. Overview. What happened Accident history Development history Technical problems Company responses Lessons learned

E N D
An Investigation of the Therac-25 Accidents Nancy G. Leveson Clark S. Turner IEEE, 1993 Presented by Jack Kustanowitz April 26, 2005 University of Maryland
Overview • What happened • Accident history • Development history • Technical problems • Company responses • Lessons learned • Ethical questions • Resources University of Maryland
What Happened • Between June 1985 and January 1987, 6 known accidents involving massive overdoses, causing death & serious injury University of Maryland
Accident History • June 3 1985: First overdose • July-Dec 1985: Two more overdoses, patient sues AECL and hospital, two requests for modifications • Jan-Feb 1986: Denial of possibility of overdose • Mar-Apr 1986: Two more overdoses, software blamed • May-Dec 1986: FDA declares Therac-25 defective, CAPs (Corrective Action Plans) sent back and forth between FDA and AECL. First Therac-25 user group meeting. • Jan 1987: Sixth overdose • Feb-July 1987: More CAPs back and forth until fifth revision of CAP sent to FDA • Nov 1988: Final safety analysis report issued Grueling first-hand descriptions of what it felt like to get a massive radiation overddose University of Maryland
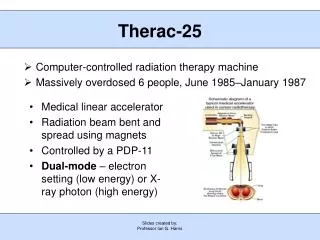
Development History • Therac-6: 6 MeV accelerator for x-rays • Therac-20: 20 MeV dual-mode (x-rays or electrons) • Separate hardware interlocks • Therac-25: 25 MeV dual-mode • All safeguards done in software • Testing • “Unit and software testing was minimal, with most effort directed at the integrated system test” • Software written in assembly on a PDP-11 University of Maryland
The Operator Interface University of Maryland
The Operator Interface • At first, operator needed to enter information at the treatment table, and then re-enter at a console in the control room • Operators complained; safeguard was removed • Error codes are reported on the screen with no English explanation • Example: (East Texas Cancer Center) “Malfunction 54” reported, caused by “dose input 2”. An AECL technician testified that “does input 2” means the dose delivered was either too high or too low (!) • “Treatment Pause” after non-critical error, which operator can ignore by pressing “P” • Causes operators to become insensitive to errors University of Maryland
Example Bugs • Data Entry Bug • Setting the bending magnets takes 8 seconds • “Delay” subroutine uses shared memory with the data entry subroutine • So data changes within 8 seconds will be wiped out when Delay exits! • Causes bugs that only show up with proficient users who do data entry in <8 seconds • Set-Up Test Bug • On every 256th pass through Set-Up (one-byte counter), the upper collimator is not checked • Problem if operator hits “set” exactly when counter rolls over to 0 • These kinds of bugs are notoriously difficult to track down University of Maryland
AECL Responses • Denial • “We did not believe that there could have been any accelerator malfunction” • Incremental, local band-aid fixes • Example: “P” key removed to prevent operators from ignoring warnings • Dragging feet, doing minimum of FDA’s requests • Perhaps justified? See ethics discussion… • Knee-jerk responses – fix the bugs as they are reported • Difficulty reproducing bugs (that only happened once in several hundred runs) University of Maryland
Lessons: General • Focusing on particular software bugs is not the way to make a safe system • Assumption that fixing one error would prevent further accidents • “There is always another software bug” • It is a bad idea to remove independent hardware interlocks, and to believe too much in software • Assume software will fail, and handle that properly, rather than trying to write “perfect” software • Don’t believe in numerical claims • “Risk assessment can be like the captured spy: if you torture it long enough, it will tell you anything you want to know” • Record the reasons for design decisions (like duplicate data entry) • Design for the worst case • Don’t enhance usability at the expense of safety • Power of user groups to cause change when companies drag their feet University of Maryland
Lessons: Software Engineering • Documentation should not be an afterthought • Establish QA practices & standards • Keep designs simple • Design audit trails and logging from the beginning • Perform extensive testing and formal analysis at the module and software level, rather than relying on system-level testing Summary of this course! University of Maryland
Ethical Questions • 500 patients treated in East Texas before first serious accident • Too much government oversight slows progress • If 1 person was getting hurt for every 1000 helped, would you take the machine out of use? How about 1:100? 1:10000? Where’s the line? University of Maryland
Resources • http://www.technology.niagarac.on.ca/courses/ctec1435/notes/Therac-25/SouthPark/01.htm University of Maryland