Download
1 / 29
290 likes | 448 Vues
Service Redesign in Tier 3 CAMHS Roz Rospopa CAMHS Regional Development Worker National CAMHS Support Service, UK. Standard.

E N D
Service Redesign in Tier 3 CAMHS Roz Rospopa CAMHS Regional Development Worker National CAMHS Support Service, UK
Standard All children and young people, from birth to their eighteenth birthday, who have mental health problems and disorders have access to timely, integrated, high quality, multi-disciplinary mental health services to ensure effective assessment, treatment and support, for them and their families.
A Comprehensive CAMHS • Underpinning Principles • Equal Access, • Partnership & Effective Commissioning, • Needs Assessment, Audit of Services, Analysis of Usage, • User & Carer Involvement, • Evidence Based, • Workforce Numbers & Competencies • Range of services • For all aged 0-18 • Age & Development / Children’s Circumstances / Learning Disability, • 24 hour cover, links with in patient services and adult services • All Tiers including early intervention and health promotion, • Full Range Evidence Based Treatments, • Local, Multi-District & Regional Commissioning
The 4-tier model for CAMHS Very specialist services, often children away from home Tier 4 Specialist Multi-disciplinary Teams Tier 3 Individual Professionals Trained in Children and Young People’s Mental Health eg Psychiatrists, Psychologists, Therapists etc Tier 2 Primary Mental Health Workers etc GPs, Paediatricians, Teachers, Health Visitors, Social Workers etc Tier 1 Four Tier Model: Together We Stand, Health Advisory Service, 1995
The 4-tier model for CAMHS: Presenting Difficulties & Projected Prevalence 0.075% = 45 Very serious problems – life threatening or very specialist treatment Tier 4 PROJECTED LOCAL PREVALENCE eg LOCAL CHILDREN’S POPULATION : 60,000 1.85% = 1110 Severe and complex problems Requiring multi-disciplinary team working Tier 3 7% = 4200 Moderately severe problems requiring attention from professionals trained in child mental health Tier 2 15% = 9000 Mild early stage problems Tier 1 Example projected local prevalence derived from: Treating Children Well, Kurtz Z., Mental Health Foundation, 1996
CAMHS Innovation projectsKey elements in a service that ‘works’For children and young people, the service should: 10 recommendations including: • Be readily accessible…. by offering home visiting and outreach, at times that can be negotiated to suit the user • Seek to engage children, young people and their parents/carers • Offer advice, consultation and training to others… • Have the capacity to keep in touch with young people over the long term…
CAMHS Innovation projectsKey elements in a service that ‘works’For children and young people, the service should: 10 recommendations including: • Effective and consistent leadership endorsed by all agencies • Strong interagency commitment over the medium to long term (steering group etc.) • Links with other services within and outside CAMHS • Retention of a stable, multidisciplinary staff group • Positive commitment to continued evaluation and audit
Key Issues in Suffolk • High Demand against Capacity • High Non Attendance: 35% Ipswich • High rate of In Patient Admission • Long length of stay within Out Patient service • Low level of Participation
The Process • Data Collection: Understand Demand • Patient Pathways: Ensure this is Fluid • Structured Interviews: Choice • Connect the Networks • Invest in the Future
Findings • Leadership • Participation • Flexibility • Workforce • Information
Clinical Challenges • Pathways • Care Bundles • Care Programme Approach • Protocol development, Transition
A Different Approach Support, Advice, Guidance Early Intervention Holistic Assessment Clinic Treatment Outreach In Patient
An Early Intervention Model • To increase Early Identification • To Support and Develop Universal Services • To reduce Stigma • To minimise Life Disruption • To Promote Problem Solving • To work together in Community Focus Clusters
Working Practice • Located in Community Cluster • Seeing the parents /carers and the child together or individually, at home or, in their preferred location. • Delivering single targeted services and working closely with other practitioners to provide multi-agency responses where appropriate • Support groups when it is helpful for people to overcome difficulties together • Parenting Groups • A CAMHS Presence in the Community
The Team 1.0 WTE per Cluster x 10 Clusters • Special Interests • Early Years • Eating Disorders • Parenting • ADHD • Adolescence • Youth Justice • Background • Nursing • Social Work • Psychology • Education
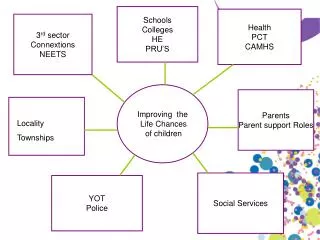
The Cluster Youth Clubs Education CAMHS High School Social Services Primary School Community Centre GP Health Visitor
The Intensive Support Team • To engage the difficult to engage. • To reduce length of in patient stay. • To form a team around the child. • To offer a flexible outreaching service • An In-Reach Service • Range of Interventions • Out of Office hours provision
Why? The Benefits • Financial • Satisfaction: supporting the connection with friends, family and school. • Promoting Resilience • Increase Choice • Facilitate a smooth transition
The Team • 1.0 WTE Clinical Team Leader • 6.5 WTE Mental Health Nurse • 0.5 WTE Clinical Psychologist • Consultant Psychiatrist support • Support Workers • Occupational Therapy
Referral Criteria • Ability to Function, acute psychiatric condition is deteriorating, risk of admission. • -OR- • Post In Patient admission to prevent the risk of relapse. • -AND- • Treatment that is more frequent and flexible in delivery is expected to be effective in preventing inpatient admission. • A safety and Support Contract can be agreed.
Clinical Presentations • Eating disorders • Psychosis • Depression • Phobias • Deliberate Self harm • Complex presentations
Developing the Evidence • Audit of caseload and activity • Monitoring of In Patient activity • Evaluation of Young Peoples experience • Development of Pathways with other services • A ‘Live’ process of Evaluation
Progress So Far • Waiting Time 8 weeks • Increase in Appropriate referrals • 10% Reduction in In Patient stay • 6% Increase in Attendance • Positive Evaluation of Satisfaction • Improved Partnership Relationships
Challenges Ahead • Workforce, Recruiting the Right People • A Choice for All • Effective Participation • Inter Agency Work: A Communication Challenge • Re- Investment in Local services
Our Challenge is not to sit around and wait until the storm blows over, but to learn how to work in the rain Pete Silas