Parathyroid Glands
340 likes | 547 Vues
Parathyroid Glands. 1849- Sir Richard Owen 1879- Anton Wölfler documented that tetany 1879-Ivar Sandstrom Hyperparathyroidism and the bone disease osteitis fibrosa cystica -1903. FELIX MANDL-1925. S uperior parathyroid glands 4 th branchial pouch

Parathyroid Glands
E N D
Presentation Transcript
1849- Sir Richard Owen • 1879- Anton Wölfler documented that tetany • 1879-Ivar Sandstrom • Hyperparathyroidism and the bone disease osteitis fibrosa cystica -1903
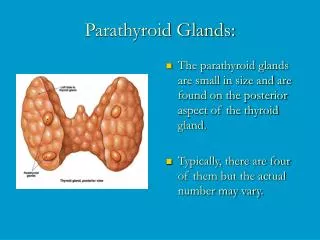
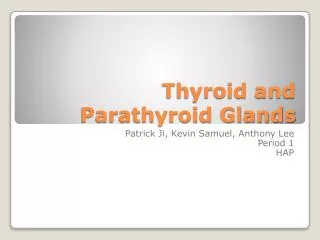
Superior parathyroid glands 4th branchial pouch • Inferior parathyroid glands -3rd branchial pouch • 80% of these glands - posterior aspect of the upper and middle thyroid lobes, cricoid cartilage • 1% of normal upper glands may be found in the paraesophageal or retroesophageal space
Common location of inferior glands is within a distance of 1 cm from a point centered where the inferior thyroid artery and recurrent laryngeal nerve cross. • 15% of inferior glands are found in the thymus. Skull base, Angle of the mandible, Superior to the superior parathyroid glands, Along with an undescended thymus
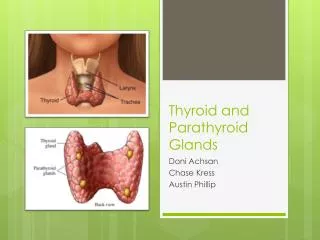
ANATOMY • 4 Parathyroid glands • 2 superior, 2 inferior • Superior parathyroid -dorsal to RLN at cricoid cartilage • Inferior parathyroid are ventral to RNL • Parathyroid glands are gray and semitransparent in newborns • Golden-yellow to light-brown in adults.
5 to 7 mm in size • Weigh approximately 40 to 50 mg each • Blood supply : branches of the inferior thyroid artery. Branches from the thyroidea ima, vessels to the trachea, esophagus, larynx, and mediastinum . The parathyroid glands drain ipsilaterally by the superior, middle, and inferior thyroid veins.
Hyperparathyroidism • is due to increased activity of parathyroid (hypercalcemia) • Types • Primary • Secondary • Tertiary
Primary -unstimulated , high, PTH secreation due to primary hyperplasia/adenoma • Secondary -chronic hypocalcemia CRF, malabsorption, vid D deficiency rickets • Tertiary - autonomous reactive hyperplasia (renal transplantation)
C/F • Bones,Stones, Abdominal groans & psychic moans • common in females 4:1 • age 20-60 , 5th decay • incidence 1:10000 • manifestation; asymptomatic >50% • behavioural problems • osteitis fibrosa cystica (von recklinghausen disease) single or multiple cyst pseudo tumour in jam, skull, middle phalanges
B/L multiple renal caliculi • peptic ulcer, pancreatitis , MEN1 syndrome • skin necrosis, band keratopathy, pseudo gout, myalgia, arthralgia, glycosuria, hypertension
Investigation Se.calcium, phosphate, albumin Se.PTH assay Alkaline phosphatase X-ray of bones TO LOCALISE PARATHYROID GLAND USG neck Thallium & technetium scan Selective venous sampling for PTH Sestamibi scanning
Differential diagnosis Secondaries in bone Multiple myeloma Vit-D intoxication Sarcoidosis paraneoplastic syndrome Familial hypocalciuric hypercalcaemia
Medical Management Primary HPT • EstrogenEstrogen– Dose required is high • SERMs – Reduction in serum calcium and markers of bone turnover after 4 weeks • BisphosphonatesBisphosphonates – Studies have shown increase in lumbar spine andfemoral neck mineral density • Calcium/Vitamin DCalcium/D • CalcimimeticCalcimimeticagents (agents CinacalcetCinacalcet) – Under investigation for primary HPT
All symptomatic • If AssymptomaticAssymptomatic Markedly elevated serum CaMarkedly Ca H/o episode lifeH/life-threatening hypercalcemia Reduce renal functionReduce function Kidney stone on RadiographKidney Radiograph Markedly elevated urinary Ca excretionMarkedly excretion Substantially reduce bone massSubstantially mass
serum calcium > 1mgserum 1mg/dL above normal • history of life threatening hypercalcemiahypercalcemia • abnormal serum Cr • elevated urine calcium, > 400mgelevated 400mg/day • kidney stoneskidney stones • < 50 years old< old • bone density less than two standard deviations below the normbelow norm • neuromuscular symptomsneuromuscular symptoms
Surgical Management • Adenoma – Unilateral vs. Bilateral Exploration – rPTH vs. Frozen Section • Hyperplasia/Multiple adenomata – Subtotal – less hypocalcemia – Subtotal w/ autotransplantation – MEN, Renal Failure – Total w/ Cryopreservation – up to 1 year
Autotransplantation • Iced saline bath • 20 20-30 mg; 10 10-20 1 1-2 mm slices • SCM vs. Brachioradialis • Pockets marked with clips • Up to 50% failure rate