TIMI 30: The PROTECT Trial
90 likes | 320 Vues
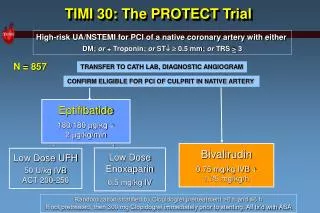
TIMI 30: The PROTECT Trial. High-risk UA/NSTEMI for PCI of a native coronary artery with either DM; or + Troponin; or ST 0.5 mm; or TRS > 3. N = 857. TRANSFER TO CATH LAB, DIAGNOSTIC ANGIOGRAM. CONFIRM ELIGIBLE FOR PCI OF CULPRIT IN NATIVE ARTERY . Eptifibatide

TIMI 30: The PROTECT Trial
E N D
Presentation Transcript
TIMI 30: The PROTECT Trial High-risk UA/NSTEMI for PCI of a native coronary artery with either DM; or + Troponin; or ST 0.5 mm; or TRS > 3 N = 857 TRANSFER TO CATH LAB, DIAGNOSTIC ANGIOGRAM CONFIRM ELIGIBLE FOR PCI OF CULPRIT IN NATIVE ARTERY Eptifibatide 180/180 mg/kg + 2 mg/kg/min + + Bivalirudin 0.75 mg/kg IVB + 1.75 mg/kg/h Low Dose Enoxaparin 0.5 mg/kg IV Low Dose UFH 50 U/kg IVBACT 200-250 Randomization stratified by Clopidogrel pretreatment >6 h and ≤6 h If not pretreated, then 300 mg Clopidogrel immediately prior to stenting. All tx’d with ASA
Association of Holter Monitor Findings with Death / MI HSC Symposium ACC 2005 p < 0.001 p < 0.001 Death or MI (%) Mean Duration of Ischemia (minutes) n=55 n=711 n=76 n=732 Ischemic event on Holter No Ischemic Event on Holter Death or MI No Death or MI
Time from First Eptifibatide Bolus to Major or Minor Bleeding HSC Symposium ACC 2005 Median time from first bolus to bleed = 7.0 hrs, IQ 3.1-14.0 N=16 bleeds Time from first bolus to bleed (hours) Kirtane, Murphy, and Gibson
Relation of Creatinine Clearance toMajor or Minor Bleeding with Eptifibatide HSC Symposium ACC 2005 n=18 n=548 p=0.01 Bleed: Median CrCl 74.6, IQ 55.3-100.1 No bleed: Median CrCl 95.5, IQ 72.1-121.0 CrCl (ml/min) Kirtane, Murphy, and Gibson
Relation of Serum Creatinine toMajor or Minor Bleeding with Eptifibatide HSC Symposium ACC 2005 n=18 n=548 p=0.49 Bleed: Median Creatinine 1.0 IQ 0.9-1.2 No bleed: Median Creatinine 1.0, IQ 0.8-1.1 Kirtane, Murphy, and Gibson Serum Creatinine (mg/dL)
Relation of Age toMajor or Minor Bleeding with Eptifibatide HSC Symposium ACC 2005 n=18 n=555 p=0.002 Bleed: Median age 69 years No bleed: Median age 59 years Age Kirtane, Murphy, and Gibson
Frequency of Non-Cr Cl Dose Adjusted Infusion Among Patients with Reduced Renal Function in PROTECT HSC Symposium ACC 2005 P=0.51 N=35 N=32 Per the protocol, the infusion dose was to be reduced for patients with CrCl50 ml/min (Eptifibatide) or CrCl<60 ml/min (Bivalirudin) Kirtane, Murphy, and Gibson
Relation of Dose Adjustment of Eptifibatide Infusion to Bleeding Outcomes HSC Symposium ACC 2005 Major/Minor Bleeding Transfusion P=0.028 P=0.009 CrCl>50 CrCl50 CrCl50 CrCl>50 % Transfusion % Major / Minor Bleeding N=17 N=18 N=530 N=17 N=18 N=530 No bleeding events or transfusions occurred among patients with CrCl50 ml/min who received a reduced-dose infusion Kirtane, Murphy, and Gibson
Bleeding in PROTECT HSC Symposium ACC 2005 • Half the bleeds occurred after 6 hours of infusion • Increasing age and a failure to dose-adjust the eptifibatide infusion in patients with reduced Creatinine Clearance (CrCl) 50 mg/dL (not Cr or weight) were the strongest independent correlates of bleeding events • A failure to adjust the eptifibatide dose for CrCl rather than Cr occurred in 17/35 (48.5%) of patients with reduced CrCl, and this was associated with a five-fold greater incidence of bleeding events (17.7% vs. 2.7%, p=0.014)