Download
1 / 30
300 likes | 451 Vues
Evaluation of Clinical Benefit in Sarcomas: Modern Imaging Modalities. Robert S. Benjamin, M.D. Department of Sarcoma Medical Oncology The SARCOMA Center. Thank you for your support!. Responders always live longer than “non-responders” unless they die of toxicity. FREIREICH’S LAW #9.

E N D
Evaluation of Clinical Benefit in Sarcomas: Modern Imaging Modalities Robert S. Benjamin, M.D. Department of Sarcoma Medical Oncology The SARCOMA Center
Responders always live longer than “non-responders” unless they die of toxicity. FREIREICH’S LAW #9
Survival vs. Time with Hematological Improvement Acute Lymphocytic Leukemia, ages 0-19 100 Hematological Improvement Hematological Improvement minus duration of Improvement 80 No Hematological Improvement 50 % Surviving 20 0 0 2 4 6 8 10 12 14 16 18 20 Months Freireich, et al: J Chron Dis 14:593-608, 1961
Time to Treatment Failure in GIST by WHO Response at 4 weeks 1.0 >50% Response 0.8 0.6 <50% Response Proportion Failure-Free 0.4 0.2 Logrank p=0.96 0.0 0 5 10 15 20 Van den Abbeele Time (Months)
p = 0.1 Response Rate 45% Time to Treatment Failure in GIST by best Response by RECIST
Responders always live longer than “non-responders” unless they die of toxicity. Corollary: If not, you have not defined response correctly. FREIREICH’S LAW #9
p = 0.1 p = 0.0002 Response Rate 45% Response Rate 83%
We Should Desist Using RECIST at Least in GIST Robert S. Benjamin, M.D. Department of Sarcoma Medical Oncology The SARCOMA Center
I-A distinct subjective benefit with favorable objective changes (% not specified) in all measurable criteria for 1 month or more. I-B objective regression of >50% for 1 month or more in a relatively asymptomatic patient. Karnofsky Criteriafor Partial Response Karnofsky DA: Meaningful clinical classification of therapeutic responses to anticancer drugs. Clin Pharmacol Ther 2: 709, 1961.
Surrogate marker for meaningful endpoint such as survival or time to progression. Objective, Quantifiable, Reproducible Criteriafor Objective Response Karnofsky DA: Meaningful clinical classification of therapeutic responses to anticancer drugs. Clin Pharmacol Ther 2: 709, 1961.
I-A distinct subjective benefit with favorable objective changes (% not specified) in all measurable criteria for 1 month or more. I-B objective regression of >50% for 1 month or more in a relatively asymptomatic patient. Karnofsky Criteriafor Partial Response Karnofsky DA: Meaningful clinical classification of therapeutic responses to anticancer drugs. Clin Pharmacol Ther 2: 709, 1961.
>50% decrease in the sum of the products of perpendicular diameters of all measurable disease Absence of appearance of any new lesions WHO Criteriafor Partial Response WHO handbook for reporting results of cancer treatment. Publication No. 48. Geneva. 1979. Miller et al. Cancer 47: 207-214, 1981
>30% decrease in the sum of the single maximum diameters of all measurable disease Absence of appearance of any new lesions RECIST (Response Evaluation Criteria in Solid Tumors)Partial Response Therase et al. JNCI 92: 205-216, 2000
Standardization and simplification No major discrepancy in the meaning and the concept of partial response to compare past and future results Not meant to discourage the development of new tools that may provide more reliable surrogate end points RECIST (Response Evaluation Criteria in Solid Tumors)Partial Response Therase et al. JNCI 92: 205-216, 2000
I-A distinct subjective benefit with favorable objective changes (% not specified) in all measurable criteria for 1 month or more. I-B objective regression of >50% for 1 month or more in a relatively asymptomatic patient. Karnofsky Criteriafor Partial Response Karnofsky DA: Meaningful clinical classification of therapeutic responses to anticancer drugs. Clin Pharmacol Ther 2: 709, 1961.
Bonadonna: Adriamycin Karnofsky Criteria (Cancer Res. 30: 2572-2582, 1970) 25% Reduction (Tumori. 60: 373-391, 1974) Jaffe: High-Dose Methotrexate (Cancer. 30: 1627-1631, 1072) 25% Reduction asPartial Response
“In the past, some groups and investigators have reported decreases of less than 50% in tumour size, but it is often not possible to determine this with precision.” Ref. Moertel and Hanley WHO Criteriafor Partial Response WHO handbook for reporting results of cancer treatment. Publication No. 48. Geneva. 1979. Miller et al. Cancer 47: 207-214, 1981
12 solid spheres covered by foam rubber up to 1.5 inches thick 2 were identical and 2 others almost identical 16 experienced clinicians False positive responses: 25% reduction - 25% 50% reduction - 6.8% Moertel and Hanley25% vs. 50% Cancer 38: 388-394, 1976
Effects of Imatinib on GIST:CT findings Baseline 8 Weeks
“We may differ about whether a patient qualifies for response, but we can all identify disease progression” What about Progression? Verweij, Aarhus, April 2001
>25% increase in the sum of the products of perpendicular diameters of all measurable disease Appearance of any new lesions If progressive disease exists in any lesion or when a new lesion appears, then the overall result will be “progressive disease.” WHO Criteriafor Progressive Disease WHO handbook for reporting results of cancer treatment. Publication No. 48. Geneva. 1979. Miller et al. Cancer 47: 207-214, 1981
“The use of a 25% increase in one or more measurable lesions or appearance of a new lesion is recommended for defining progression of disease. This percentage should not necessarily be regarded as influencing the management of the patient.” WHO Criteriafor Progressive Disease WHO handbook for reporting results of cancer treatment. Publication No. 48. Geneva. 1979. Miller et al. Cancer 47: 207-214, 1981
>20% increase in the sum of the single maximum diameters of all measurable disease Appearance of any new lesions No comment about one or more areas of clear progression. RECIST (Response Evaluation Criteria in Solid Tumors)Progressive Disease Therase et al. JNCI 92: 205-216, 2000
Standardization and simplification No major discrepancy in the meaning and the concept of partial response to compare past and future results Major discrepancy in the meaning and the concept of Progressive Disease prohibiting comparison past and future results RECIST (Response Evaluation Criteria in Solid Tumors)Progressive Disease Therase et al. JNCI 92: 205-216, 2000
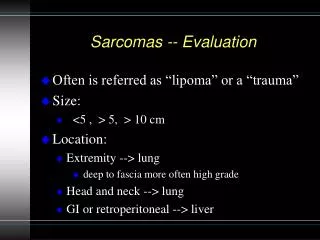
Osteosarcomas may not shrink. Sarcomas can become fibrotic, cystic, or myxoid and not change in overall size substantially. Inaccurate response definitions may explain partially why prognostic factors for response and survival are different Size may not Matter
PET for metabolic activity. Dynamic Contrast-Enhanced MRI (or CT) for vascular changes. Better use of standard contrast-enhanced CT. What about Functional Imaging?
Explore the role of modern imaging in the evaluation of benefit or lack of benefit for sarcomas. Discuss the data over dinner after a break for the CTOS mixer. Reach a consensus on new, improved, criteria for response. Find a name. Publish our criteria. Challenge for this Symposium
RECIST is a great name, but common usage of RECIST (Response Evaluation Criteria in Solid Tumors) Criteria is redundant. New Names: CTOS Criteria SARC Criteria Mixture: CTOS-SARC or SARC-CTOS REIS (Response Evaluation in Sarcomas) Criteria Could be modified for other solid tumors to REIST Criteria ERIS (Evaluating Response in Sarcomas) Criteria Could be modified for other solid tumors to ERIST Criteria What’s in a Name?
Evaluation of Clinical Benefit in Sarcomas: Modern Imaging Modalities Robert S. Benjamin, M.D. Department of Sarcoma Medical Oncology The SARCOMA Center