Download
1 / 1
40 likes | 374 Vues
Endometrial large cell neuroendocrine carcinoma : a case report Reina Sato, Aiko Kawano, Hiroyuki Shigeta Department of Obstetrics and Gynecology, Yokohama Municipal Citizen’s Hospital, Yokohama, Japan. Objectives. Results. Conclusions. Postoperative diagnosis:

E N D
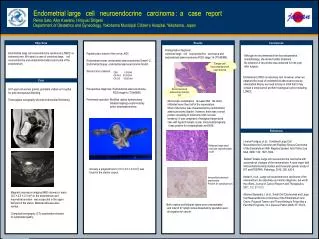
Endometrial largecellneuroendocrinecarcinoma: acasereport Reina Sato, Aiko Kawano, Hiroyuki Shigeta Department of Obstetrics and Gynecology, Yokohama Municipal Citizen’s Hospital, Yokohama, Japan Objectives Results Conclusions Postoperative diagnosis: combined largecellneuroendocrinecarcinoma and endometrioidadenocarcinoma FIGO stage 1b (T1bN0M0). Endometrial large cell neuroendocrine carcinoma (LCNEC) is extremely rare. We report a case of combined largecellneuroendocrine and endometrioid adenocarcinoma of the endometrium. Papanicolaou smear of the cervix: AGC Endometrial smear: endometrial adenocarcinoma Grade1-2. Endometrial biopsy: endometrial adenocarcinoma Grade1. Serum tumor markers: Preoperative diagnosis: Endometrioidadenocarcinoma, FIGO stage1b (T1bN0M0). Performed operation: Modified radical hysterectomy bilateral salpingo-oophorectomy pelvic lymphadenectomy Although we recommended her the postoperative chemotherapy, she denied further treatment. No evidence of recurrence was observed for one year after surgery. Large cell neuroendocrine carcinoma CEA 3.0IU/ml CA19-9 30.3IU/ml CA125 19.9IU/ml Endomerial LCNEC is extremely rare. However, when we obtained the result of endometrioid adenocarcinoma by endometrial biopsy, we need to keep in mind that it may contain a small part of another histological cancer including LCNEC. Case A 61-year-old woman (para4, gravida4) visited our hospital for post-menopausal bleeding. Transvaginalsonography showed endometrial thichening. Endometrioidadenocarcinoma, G1 Microscopic examinationrevealed thatthe tumor infiltrated more than half of the myometrium. Most of the tumor was characterized by endometrioid adenocarcinoma Grade1, however, there was a small portion consisting of solid tumor with necrotic tendency. It was composed of malignant large-sized cells with hyperchromatic nuclei. Immunohistologically, it was positive for synaptophysin and NSE. References Lorena Posligua, et al., Combined Large Cell NeuroendocrineCrcinoma and Papillary Serous Carcinoma of the Endometrium With Pagetoid Spread. Arch Pathol Lab Med, 2008; 132: 1821-1824. TadashiTerada, Large cell neuroendocrine carcinoma with sarcomatous changes of the endometrium: A case report with immunohistochemical studies and molecular genetic study of KIT and PDGFRA. Pathology, 2010; 206: 420-5. Kedar K, et al., Large cell neuroendocrine carcinoma of the endometrium: An extremely uncommon diagnosis, but worth the efforts. Journal of Cancer Reserch and Therapeutics, 2011, 7-2: 211-213. Albores-Saavedra J, et al., Small Cell Carcinomas and Large Cell NeuroendocrineCrcinomas of the Endometrium and Cervix: Polypoid Tumors and Those Arising in Polyp May a Favorble Prognosis. Int J GynecolPathol 2008; 27: 333-9. Malignant large-sized cells with hyperchromatic nuclei Grossly, a polypoid tumor (3.5×2.5×2.1cm3) was found in the uterine corpus. Immunohistochemicalexamination: Positive for synaptophysin. Magnetic resonance imaging (MRI) showed a mass (3.0×2.5×2.1cm3) in the endometrium andmyometrial invasionwas suspected in the upper half part of the uterus. Bilateral adnexae were normal. Computed tomography (CT) examination showed no lymphadenopathy. Both ovaries and fallopian tubes were unremarkable, and total of 27 lymph nodes dissected by operation were all negative for cancer.