Eyelid Lumps and Bumps
540 likes | 2.45k Vues
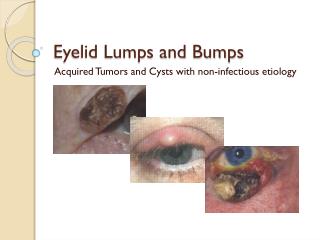
Eyelid Lumps and Bumps. Acquired Tumors and Cysts with non-infectious etiology. Benign Tumors. Actinic Keratosis What is it? Slow growing keratinization of the epithelium Results from excessive sun exposure Pre-malignant: may transform into squamous cell carcinoma Appearance

Eyelid Lumps and Bumps
E N D
Presentation Transcript
Eyelid Lumps and Bumps Acquired Tumors and Cysts with non-infectious etiology
Benign Tumors • Actinic Keratosis • What is it? • Slow growing keratinization of the epithelium • Results from excessive sun exposure • Pre-malignant: may transform into squamous cell carcinoma • Appearance • Rough, dry, and scaly plaque that is flat or slightly raised • Up to 2.5 cm diameter individually • Often multiple lesions in a single area that coalesce • Distinct boarders • May be skin colored to dark brown • Who gets it? • Elderly individuals with lightly pigmented skin • Rarely develops on the eyelid • Common on the scalp, ears, forehead, and backs of hands • The patient may notice itching or burning of the lesion
Benign Tumors • Actinic Keratosis • Management • Biopsy for definitive diagnosis • Usually frozen (cryotherapy) or excised
Benign Tumors • Squamous Cell Papilloma • What is it? • Outgrowth of fibrovascular connective tissue • Covered by irregular keratinized stratified squamous epithelium • Appearance • Variable presentations • “Skin tag” type: narrow base, pedunculated, skin colored • Board base with “raspberry like” appearance • May be difficult to differentiate from viral wart (human papillomavirus) • Who gets it? • No predilection to race or gender • Management • Removed by excision
Benign Tumors • Squamous Cell Papilloma
Benign Tumors • Basal Cell Papilloma • What is it? • Expansion of the squamous epithelium stemming from basal cell proliferation • Slow growing lesion • Appearance • Round “coin-like” lesion with “stuck-on” appearance • Up to 2.5 cm diameter • Slightly raised and crusty: often keratinized similar to actinic keratosis • Tan to dark brown in color • Variety of textures: granular to velvety • Who gets it? • Common in the elderly • Most people develop at least one during their lives • Usually develop on the head, neck, or trunk • Management • No treatment required except for cosmetic reasons or if they become irritated • Removed by excision
Benign Tumors • Basal Cell Papilloma
Benign Tumors • Inverted Follicular Keratosis • What is it? • Rare and often rapid growing lesion arising from a hair follicle • Histologically similar to basal cell papilloma, but with deeper extension into the dermis • Appearance • Non pigmented papilloma at the lid margin • Up to 1 cm diameter • Who gets it? • Typically older males • Management • Deep excision • Recurrence is common if not completely removed
Benign Tumors • Inverted Follicular Keratosis
Benign Tumors • Keratoacanthoma • What is it? • Rare and rapidly growing variant of actinic keratosis • Also pre-malignant, potentially transforming into squamous cell carcinoma • Appearance • Initially appears as a pink hyperkeratotic lesion usually on the lower lid • After a period of rapid growth, remains stable for several months • Then begins to involute and a keratin filled crater often forms • Complete involution can occur after a year leaving a residual scar • Who gets it? • Same demographic as actinic keratosis • Higher occurrence in patients on immunosuppressive therapy following kidney transplants • Management • Usually excised • Occasionally treated with cryotherapy or radiotherapy
Benign Tumors • Keratoacanthoma
Benign Tumors • Melanocytic Nevus • What is it? • Tumor composed of cells derived from either epidermal or dermal melanocytes • Acquired and congenital forms • Generally low to no malignant potential • Appearance • Junctional: Uniform brown macule or plaque • Compound: Uniform, light to dark brown, raised papule • Intradermal: Papillomatous with little to no pigment. Associated with dilated vessels and protruding lashes • Who gets it? • Junctional type occurs in the young • Compound type occurs in middle age • Intradermal type most common overall and occurs in the elderly • Management • Removal for cosmetic reasons or if malignancy is suspected • Excision may need to be followed by reconstruction depending on location and size
Benign Tumors • Melanocytic Nevus Junctional Nevus Compound Nevus Intradermal Nevus
Benign Tumors • Xanthelasma • What is it? • Aggregation of lipid filled macrophages at the level of the dermis • Common and frequently bilateral • Appearance • Yellowish subcutaneous plaque • Usually on the medial portion of the eyelids • Often multiple • Who gets it? • Middle aged and the elderly • May be associated with elevated cholesterol especially when occurring in younger individuals and with corneal arcus • Management • Removed for cosmetic reasons • Usually treated with carbon dioxide or argon laser • May be excised • Recurrence suggests persistently elevated cholesterol
Benign Tumors • Xanthelasma
Benign Tumors • Pilomatricoma • What is it? • Abnormal proliferation of the germinal matrix cells in a hair follicle • Frequently becomes calcified • Appearance • Deep nodule • Becomes hard if calcified • Who gets it? • Common in young females • Management • Excision
Benign Tumors • Pilomatricoma
Benign Tumors • Neurofibroma • What is it? • Abnormal proliferation of Schwann cells, fibroblasts, and axons • Appearance • Characteristic S shaped lesion • Typically located on the upper lid • Who gets it? • Solitary lesions occur in adults • 25% associated with neurofibromatosis-1 • Children with neurofibromatosis-1 are affected by diffuse lesions • Management • Solitary lesions removed by excision • Diffuse lesions are more difficult to remove
Benign Tumors • Neurofibroma
Malignant Tumors • Basal Cell Carcinoma • What is it? • Locally invasive proliferation of pluripotent epidermal basal cells • Most common human malignancy and most common eyelid malignancy • Slow growing with no metastatic potential • Appearance • Usually on the lower eyelid • Non-tender ulceration • Irregular boarders • Possible keratinization • Destruction of eyelid architecture • Nodular type: pearl like appearance with dilated blood vessels on surface • Noduloulcerative type: central ulcer with raised pearly edges • Sclerosing type: lateral, hardened, infiltration beneath the epidermis. May be confused with chronic blepharitis
Malignant Tumors • Basal Cell Carcinoma • Who gets it? • Common in the elderly • Risk factors include fair skin and high cumulative sun exposure • Management • Diagnosis confirmed with biopsy • Excision is the common removal technique • Mohs micrographic surgery removes the tumor along with a thin layer of surrounding tissue. The surround is immediately examined for tumor cells and the procedure repeated if any are found. Highest cure rate at 98%. • Recurring tumors tend to be more invasive and difficult to treat
Malignant Tumors • Basal Cell Carcinoma Nodular Ulcerative Sclerosing
Malignant Tumors • Squamous Cell Carcinoma • What is it? • Proliferation of invasive cells arising from the squamous cell layer of the epidermis • Can arise de novo or from existing actinic keratosis or keratoacanthoma • Less common, but more aggressive than basal cell carcinoma • Lymph node metastasis in 20% of cases • Appearance • Variety of appearances and may be difficult to distinguish from BCC • Scaly with irregular boarders • Absence of surface vasculature • Extensive keratinization usually present • Lesions may bleed • Nodular type: keratinized nodule that develops erosions and fissures • Ulcerating type: everted boarders with a red, well defined base • Cutaneous horn: invasive growth underlies keratin horn
Malignant Tumors • Squamous Cell Carcinoma • Who gets it? • Most common occurrence is in the elderly • Risk factors include fair skin, sun exposure, and immune suppression • Management • Can be fatal if left untreated (2,500 annual deaths in USA) • Confirmed with biopsy • Mohs micrographic surgery: highest cure rate 94-99% • Other options include standard scalpel excision, cryotherapy, and radiotherapy
Malignant Tumors • Squamous Cell Carcinoma Nodular Ulcerative Cutaneous horn Large ulcerative
Malignant Tumors • Sebaceous Gland Carcinoma • What is it? • Slow growing tumor • Arises from the meibomian glands, glands of Zeis, or sebaceous glands in the caruncle • More likely to occur on the upper lid where glands are more numerous • Appearance • No pathognomonic presentation • Initially can appear similar to chalazion or chronic blepharitis • Yellowish material may be seen within the tumor • Nodular type: hard, painless, immobile nodule similar to chalazion • Spreading type: thickened lid margin, loss of lashes, similar to chronic blepharitis
Malignant Tumors • Sebaceous Gland Carcinoma • Who gets it? • Females in their 60's and 70's most commonly affected • Youngest reported case was in a 3 year old • Management • Because of appearance, diagnosis is often delayed • Mortality rate is 5-10% • Large (1cm) and non-resolving chalazion should be suspected • Cryotherapy and surgical excision are the standard treatments • Recurrence is as high as 33% • Little documentation for Mohs, but possibly lower recurrence rate
Malignant Tumors • Sebaceous Gland Carcinoma Nodular Spreading Conjunctival involvement
Malignant Tumors • Melanoma • What is it? • Epidermal and dermal proliferation of transformed and invasive melanocytes • Arises from existing nevus, lentigo maligna (pre-malignancy), or de novo • High potential for metastasis • Potentially fatal (represents greater than 2/3 of all skin cancer deaths) • Appearance • Rarely develops on the eyelid (1% of all eyelid lesions) • Half of those that do are non-pigmented • Asymmetric plaque or nodule • Irregular and indistinct boarders • Variable colors in the lesion (blue and black) • Diameter larger than ~6mm • Associated with destruction of local anatomy and loss of lashes
Malignant Tumors • Melanoma • Who gets it? • Most common in elderly individuals with light skin • History of sun damaged skin • Management • Question any new, changing, or irregular appearing lesions • Melanoma confirmed with biopsy • Wide surgical excision with up to a 1 cm margin for confirmed malignancy • Local lymph node dissection if malignancy is more than 1.5 mm deep • Prognosis and recurrence is tied to size and any metastasis of original lesion • Patients should be followed closely following surgery
Malignant Tumors • Melanoma
Malignant Tumors • Merkel Cell Carcinoma • What is it? • Very rare and fast growing form of skin cancer • Highly malignant and potentially fatal • Arises from Merkel cells located in the basal layer of the epidermis • Normal cells thought to play a regulatory role in epidermal growth • Appearance • Frequently involves the upper eyelid • Red, purple, or violet colored, well defined nodule • Wide variation in size, from less that 2cm to larger than 15cm • Overlying skin is intact
Malignant Tumors • Merkel Cell Carcinoma • Who gets it? • Average age of diagnosis is 75 • 20x more likely to occur in whites than blacks • No gender predilection • Risk factors include sun exposure and immune suppression • Management • Many have metastasized by the time they are diagnosed • CT and/or MRI imaging used to evaluate systemic spread • Primary tumor removed with a wide excision (margins up to 3cm if possible) • Chemotherapy and/or radiotherapy depending on spread • 2 year mortality rate of 30-50%
Malignant Tumors • Merkel Cell Carcinoma
Cysts • Chalazion • What is it? • AKA meibomian cyst • Fatty secretions of a meibomian gland are retained • Causes a chronic, painless inflammation • Patients with rosacea or meibomian gland dysfunction are more prone to developing multiple and recurrent chalazion • Appearance • Nodule that has enlarged gradually • May enlarge up to nearly 1 cm • If large enough, may induce astigmatism by pressing on the cornea
Cysts • Chalazion • Treatment • About one third drain and resolve spontaneously • Standard therapy aimed at stimulating and speeding draining by using warm compress and massage • Steroid injection through the palpebral conjunctiva • 0.1-0.2 ml Kenalog (triamcinolone) • 80% success rate • May cause local depigmentation of the skin • Oral tetracycline/doxycycline useful in patients with chronic lid inflammation • Do not use in children or pregnant/nursing women! • 250mg PO qid tetracycline • 100mg PO bid doxycycline • 1-2 week course • Incision and drainage through the palpebral conjunctiva and tarsal plate • Biopsy a recurrent chalazion - it may be sebaceous cell carcinoma
Cysts • Cyst of Zeis • What is it? • Variation of chalazion • Non-translucent retention cyst involving the anterior lid margin • Gland of Zeis produces oil for eye lashes
Cysts • Cyst of Moll • What is it? • Variation of chalazion • AKA Sudoriferous cyst • Translucent retention cyst involving the anterior lid margin • Variation of chalazion • Gland of Moll is a modified sweat gland also emptying to the lashes
Cysts • Epidermoid Cyst • What is it? • AKA sebaceous cyst • Cyst lined by stratified squamous epithelium and containing keratin and sebaceous material • Result from ingrowth of surface epidermis after trauma or surgery • Appearance • Round, well defined, non-tender mass • Ruptured cysts cause an acute inflammatory response and possible secondary infection • Treatment • Complete surgical excision
Cysts • Eccrine Hidrocystoma • What is it? • Rare cyst that forms from retained sweat in a blocked and dilated sweat duct • More common in females • Appearance • Similar to Cyst of Moll with the exception that it does not involve the lid margin • Painless and usually asymptomatic • May grow up to 6mm • Treatment • Monitor or needle puncture if desired
Cysts • Syringoma • What is it? • Benign and asymptomatic proliferation of sweat gland duct epithelium • Relatively common • Most common in adult females • Appearance • Multiple small (3mm or less) papules • May be skin color or yellowish • Treatment • Removed for cosmetic reasons only • No set recommended removal technique • Options include excision, cryotherapy, dermabrasion, electrocautery and more
Cysts • Milia • What is it? • Tiny epidermoid cysts that tend to occur in clusters • Result from a blocked vellus hair follicles that retain the keratin • Very common – occurs in half of all infants • May also occur following dermabrasion or damage to the follicle • Appearance • Small pearly white to yellowish papules • Treatment • No treatment necessary • Needle puncture and expression may be performed if desired
Resources • Kanski, Jack J. Clinical Ophthalmology a Systemic Approach. 6th ed. Edinburgh, UK: Elsevier, 2007. • http://www.mayoclinic.com/health/actinic-keratosis/DS00568 • http://www.consultantlive.com/photoclinic/article/10162/1265743 • http://www.skincancer.org/Basal-Cell-Carcinoma/ • http://www.skincancer.org/squamous-cell-carcinoma.html • http://emedicine.medscape.com/article/1101433-overview • http://emedicine.medscape.com/article/1213671-overview • http://emedicine.medscape.com/article/1100917-overview • http://www.ncbi.nlm.nih.gov/pmc/articles/PMC1781304/ • http://emedicine.medscape.com/article/1058063-overview • http://emedicine.medscape.com/article/1059871-overview