Left Upper Quadrant Pain and Masses
Left Upper Quadrant Pain and Masses. Presented by:- Naif Al- Rowaily Ahmed Al- Zahrani Supervised by:- Dr.bismar. Differential Diagnosis:-. 1-Splenomegaly 2-Stomach Carcinoma Gastric distension

Left Upper Quadrant Pain and Masses
E N D
Presentation Transcript
Left Upper Quadrant Pain and Masses Presented by:- Naif Al-Rowaily Ahmed Al-Zahrani Supervised by:- Dr.bismar
Differential Diagnosis:- 1-Splenomegaly 2-Stomach Carcinoma Gastric distension 3-Pancreas Pseudocyst carcinoma 4-Kidney Polycystic kidney Hydronephrosis Pyonephrosis Perinephrosis Perinephric abscess Carcinoma Tuberculosis Solitary cyst Wilm's tumour 5-Colon Carcinoma of the splenic flexure Faeces Diverticular mass
causes of LUQ abdominal pain: • Abdominal wall and ribs. Pain will occur most commonly from herpes zoster, contusion, hernia, rib fracture, or metastatic tumor. • Spleen. Painful splenic infarcts are not unusual in subacute bacterial endocarditis, polycythemia, sickle cell anemia, leukemia, periarteritis nodosa, and other autoimmune disorders. A ruptured spleen is an important consideration in abdominal injuries, particularly those in children and in patients with infectious mononucleosis. • Stomach. Acute gaseous distention of the stomach in gastritis, pneumonia, and pyloric obstruction is a common cause of LUQ pain. Gastric carcinoma that extends beyond the wall of the stomach may cause pain. Episodic obstruction of the stomach in the “cascade stomach” should be considered in the differential diagnosis. Herniation of the stomach through the diaphragm occasionally causes LUQ pain. • Colon. An inflamed diverticulum or an inflamed splenic flexure from granulomatous colitis may cause pain in the LUQ. Less commonly, the colon develops a perforating or constricting carcinoma in this area, which obstructs the bowel. A mesenteric infarct of the colon, as well as gas or impacted feces in the splenic flexure, may also cause LUQ pain. • Pancreas. Acute pancreatitis, pancreatic pseudocyst, and carcinoma of the pancreas may cause LUQ pain. • Adrenal gland. Adrenal infarction from emboli or Waterhouse–Friderichsen syndrome may cause pain, but neoplasms rarely do until they have become massive. • Kidney. Renal infarct, renal calculus, acute pyelonephritis, and nephroptosis with a Dietl crisis may cause LUQ pain. Perinephric abscess must also be considered. • Aorta. Dissecting or atherosclerotic aneurysms of the aorta may cause LUQ pain, especially when they occlude a feeding artery to one of the structures there. • Spine. Herniated disc, tuberculosis, multiple myeloma, osteoarthritis, tabes dorsalis, spinal cord tumor, and anything else that may compress or irritate the intercostal nerve roots can cause LUQ pain.
Approach to the Diagnosis • The presence or absence of other symptoms and signs will be most helpful in the diagnosis. In acute cases, a surgeon is consulted and a flat plate of the abdomen, CBC, urinalysis, arid perhaps a serum amylase level should be done. If necessary, a CT scan of the abdomen is also done. Gastroscopy and colonoscopy may be desirable before other x-rays are done. In chronic cases, however, an upper GI series, barium enema, and stool examination for blood, ova, and parasites are indicated.
Other helpful tests: • Four-quadrant peritoneal tap (ruptured spleen) • Quantitative urine amylase • IVP (renal calculus) • Stool for occult blood (carcinoma, diverticulitis) • Gallium scan (diverticulitis, etc.) • X-ray of thoracolumbar spine (radiculopathy) • Small-bowel series (Meckeldiverticulum) • Laparoscopy (ruptured viscus or peritonitis) • Aortogram (dissecting aneurysm) • Lymphangiogram (retroperitoneal sarcoma) • Exploratory laparotomy
Causes of LUQ abdominal mass: • M—Malformations of the skin, subcutaneous tissue, fascia, and muscle are usually hernias; for the spleen, they are aneurysms; for the splenic flexure of the colon, they are mainly volvulus, intussusceptions, and diverticula. Gastric dilatation of the stomach is caused by obstruction or pneumonia. Cysts are common for the pancreas, just as polycystic disease, single cysts, and hydronephrosis are common for the kidney. There is no common malformation for the adrenal gland. • I—Inflammatory conditions of the skin, subcutaneous tissue, muscle, and fascia are usually abscesses and cellulitis. In the spleen, a host of systemic inflammatory lesions can cause enlargement (see page 482), but primary infections of the spleen are unusual. The colon may be inflamed by diverticulitis, granulomatous colitis, and, occasionally, by tuberculosis. Inflammatory disease of the stomach does not usually produce a mass, but if an ulcer perforates or if a diverticulum ruptures, a subphrenic abscess may form in the left hypochondrium. Inflammatory pseudocysts may form in the tail of the pancreas. A palpable perinephric abscess and an enlarged kidney from acute pyelonephritis or tuberculosis may be felt, but inflammatory lesions of the adrenal gland are rarely palpable. • N—Neoplasms of the organs mentioned above account for most of the masses in the LUQ. Carcinoma of the stomach or colon, Hodgkin disease, chronic leukemias involving the spleen, Wilms tumor, carcinoma of the kidney, and neuroblastoma must be considered. A retroperitoneal sarcoma is occasionally responsible for an LUQ mass. • T—Trauma to the spleen or kidney will produce a tender mass in the LUQ. Less common traumatic lesions here include contusion of the muscle and perforation of the stomach or colon. It should be noted that the left lobe of the liver may project into the LUQ; therefore, tumor and abscess of the liver must be considered.
Approach to the Diagnosis • The presence or absence of other symptoms and signs is the key to the clinical diagnosis of an LUQ mass. The presence of jaundice would suggest the mass is a large spleen. The presence of blood in the stool would suggest carcinoma of the colon. The presence of hematuria would suggest the mass is renal in origin. An enema should be done to exclude fecal impaction before an extensive workup is performed. • A conservative workup will include a CBC, sedimentation rate, urinalysis, chemistry panel, platelet count, stool for occult blood, coagulation profile, and a flat plate of the abdomen. On the basis of these results, the clinician can determine whether to do an upper gastrointestinal (GI) series, barium enema, IVP, or CT scan of the abdomen. Another approach would be to do the CT scan immediately. In the long run, the latter approach may be more cost-effective. It is usually prudent to get a surgical or gastroenterology consult to help decide between the two approaches.
SPLEENOMEGALY Causes :- Infective:- Bacterial Typhoid Typhus Tb Septicaemia Abscess Viral Glandular fever Spirochaetal syphilis Leptospirosis Protozoal malaria leishmania Parasitic hydatid cyst Inflammatory:- Rheumatoid arthritis Sarcoidosis Lupus Amyloid
Cont’d. Neoplastic:- Leukaemia Lymphoma Polycythaemia vera Myelofibrosis Primary tumours Metastases Haemolytic disease:- Anemia Hereditary spherocytosis Acquired haemolytic anaemia Thrombocytopenic purpura Storage diseases:- Gaucher's disease Deficiency diseases:- Pernicious anaemia Severe iron-deficiency anaemia splenic vein hypertension:- Cirrhosis Splenic vein thrombosis Portal vein thrombosis Non-parasitic cysts
Another Case?? This boy exhibits splenomegaly, distended abdomen and severe muscle wasting. What do you think? Your diagnosis!
SPLEEN-anatomy: • The spleen is a friable blood-filled organ lying in the left upper quadrant of the abdomen behind the 9th, 10th and 11th ribs It oval shaped and has a notched anterior border. • It weighs about 150 g, is ellipsoid in shape and lies with its long axis along the line of the 10th rib. • Supplied by Large splenic artery, which is the largest branch of the Celiac artery, and short gastric arteries that arise from the gastroepiploic arteries. • The splenic vein leaves the hilum and run behind the tail and the body of the pancreas.( Joins the S.M.V to form the Portal vein). • The nerves accompany the Splenic artery and are derived from the Celiac plexus.
Function: • The Function of the human spleen is to filter abnormal RBCs, stores platelets, produce tuftsin and properdin (opsins) produces antibodies(IgM) and is site of phagocytosis . • During fetal development the spleen produces red blood cells. • By the fifth month of gestation the spleen no longer has hematopoietic function but retains the capacity throughout life. • Red cells that pass through the spleen undergo a “cleaning” or repair.
The spleen is the site of destruction in autoimmune disease. Also is involved in specific and nonspecific immune responses (promotes phagocytosis and destruction of bacteria). About 20% of people have an accessory spleen, and 33% of total body platelets are stored in the spleen. The spleen is the most common intraabdominal organ injured in blunt trauma.
Splenomegaly:- The spleen must be enlarged to about three times its normal size before it becomes clinically palpable. The lower margin may feel notched on palpation also the spleen may become so massive in size that it is palpable in the right iliac fossa. Massive splenomegaly is likely to be due to chronic myeloid leukaemia, Myelofibrosis or lymphoma. Splenomegaly may lead to hypersplenism ( pancytopenia as cells become trapped in an overactive spleen and are destroyed). So anaemia, infection, or haemorrhage may result.
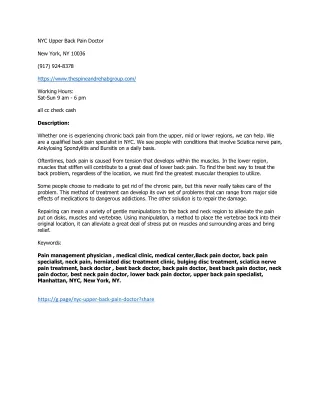
Palpation for the lower edge of the spleen In adults the spleen tends to enlarge diagonally from the left hypochondrium to the RIF. You should ask the patient if they can turn slightly on to their right side. With your non-examining hand, you should also splint the left lower ribs from behind, to fix the spleen, making it more easy to palpate anteriorly. While coordinating with the patients respiratory cycle, gradually move from the RIF to the left hypochondrium. As with the liver, you are feeling for the edge of the spleen.
Hypersplenism • Refers to a variety of ill effects resulting from increased splenic function that may be improved by splenectomy. • The criteria for diagnosis included: • Anemia, leukopenia, thrombocytopenia or a combination of the three . • Compensatory bone marrow hyperplasia. • Splenomegaly. • Hypersplenism can be categorized as primary or secondary.
Hyposplenism • Is a potentially lethal syndrome characterized by diminished splenic function. • The patient peripheral blood smears appear as if they are asplenic. • Hyposplenism can occur in the presence of abnormal sized or enlarged spleen. • The danger of hyposplenism is the risk of developing potentially lethal sepsis. • Sickle cell anemia is the most common disease associated with hyposplenism. • Themost common surgical disease associated with hyposplenism is chronic UC.
Anemia • Hemolytic anemia results from an increase in the rate of red blood cell destruction. • Many hemolytic anemias have a hereditary basis • Congenital hemolytic anemias have defects in the cell membrane, cell structure or problems with hemoglobin structure or synthesis (G-6-PD) • Acquired hemolytic anemias have factors attached to the outside cell structure.
Sickle Cell Anemia • Symptoms • Severe abdominal pain. • Signs of peritoneal irritation. • Chronic features : • Retarded growth and development, bone and joint problems , cardiovascular, pulmonary, hepatobiliary, genitourinary, and neurologic manifestations, hematuria, priapism and ulcerations over the distal portions of the legs. • The incidence of pigmented gallstones increases with age.
Sickle Cell Anemia • Diagnosis • Characteristic sickle cells on blood smear. • Hemoglobin electrophoresis. • Treatment • Palliative-directed towards minimizing complications of the disease. • Many patients die during childhood from infections, renal failure and heart failure.
Sickle Cell Crisis • Splenic involvement • Is unknown or unclear. • During a crisis the spleen sequesters a large volume of blood – to the point of hypovolemia. • Hypovolemic shock and death may occur within hours. • So treat them as Shock pts with ABCs and they may need splenoctomy after they become stable.(?)
Thalassemia • These hereditary hemolytic anemia’s result from a defect in hemoglobin synthesis. • Beta thalassemia is the most common type. • Hemoglobin electrophoresis in thalassemia major reveals a absence of hemoglobin A and an increase in hemoglobin F. • Treatment includes transfusions, iron chelation and splenectomy.
Autoimmune Hemolytic Anemia • Is an acquired hemolytic anemia resulting from antibodies that are produced by the body against its own red cells. • Patients have hemolysis with anemia, reticulocytosis, shortened erythrocyte lifespan, fluctuating jaundice and splenomegaly. • The distinguishing feature is a positive direct Coombs test-this identifies antibodies on the red cell surface • The type of antibody attached to the red cell determines the mechanism of hemolysis
Autoimmune Hemolytic Anemia • Drugs can be associated or related to this anemia • Penicillin, cephalothin, streptomycin, methyldopa, quinidine, aspirin, phenacetin and several sulfonamides • Pallor and splenomegaly are the main physical findings. • Treatment is directed towards the hemolytic anemia and any underlying disease. • Blood transfusion, steroids and splenectomy are often used.
Idiopathic(autoimmune) Thrombocytopenic Purpura Thrompocytopenia results from immune destruction of platelets.
Chronic ( adult –type ) ITP • Most common cause of isolated thrombocytopenia • diagnosis of exclusion. • Idiopathic but may occur with autoimmune disorders e.g : SLE , thyroid disease , chronic lymphocytic leukemia ,HIV or the same drugs that cause autoimmune hemolytic anaemia
Pathophysiology - IgGautoantibody -Spleen : - site of antibody production & platelet destruction. -Usually not palpable (enlarged in 10 % )
Clinical presentation - insidious onset - May be seen after mild viral illness or after immunization - Mucosal or skin bleeding - Petechia and easy bruising - Hematuria - Melena - Epistaxis - Female with menorrhagia
Laboratory results - Peripheral blood film : ↓ platelet , large platelets - Bone marrow : plentiful megakaryocytes critical test to rule out other causes of thrombocytopenia - Anti-platelet antibodies present in most . - ↑ bleeding time - PT & PTT normal
MANAGEMENT • Conservative if mild • - steroids • - splenoectomy if steroids fail * has 60 % cure rate • IV gamma globulin if steroids and splenoectomy fail or rapid response is required • others: prednisolone, platelets , plasma exchange ,danazol
Prognosis - Fluctuating course • Overall relatively benign , mortality 1-2 % - Major concern is cerebral hemorrhage at platelets count < 5 ×10^9 /L
Cysts and Tumors of the Spleen • The differential diagnosis of splenomegaly should include splenic masses and primary tumors (these conditions are rare however they must be considered) • Cystic lesions comprise parasitic and nonparasitic cysts:- • Parasitic cysts are due almost exclusively to echinococcal disease (rare disease) • Nonparasitic cysts are classified as primary (true) which have an epithelial lining or pseudocysts (more common) • Symptoms of splenic cysts are vague and are caused primarily by mass effect (compression of adjacent viscera)
Cysts and Tumors of the Spleen • Selected nonparasitic cyst may be managed by aspiration. • Splenectomy should be performed for all large cyst and those with an uncertain diagnosis. • Malignant and benign primary tumors of the spleen are rare. • Most primary malignant tumors are angiosarcomas.
Infectious Mononucleosis • A disease characterized by fever, sore throat, lymphadenopathy and atypical lymphocytes. • Most patients are young. • Clinical symptoms are similar to those of a severe upper respiratory tract infection. • The spleen is enlarged and palpable in over 50% of patients. • Splenic rupture may occur.
Incidental Splenectomy • The spleen is vulnerable to injury during operative procedures in the upper abdomen. • When the splenic capsule is torn, splenectomy is frequently performed. • Morbidity and mortality is higher with iatrogenic injury requiring splenectomy.