Download
1 / 35
350 likes | 513 Vues
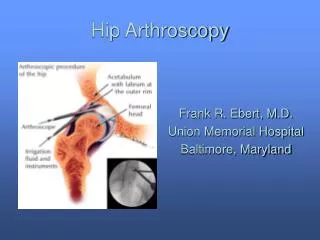
Health Care for Adolescents and Adults with Down Syndrome 1 st India International Conference on Down Syndrome September 2017. George T Capone, M.D. Kennedy Krieger Institute, Baltimore Maryland. Persons with Down syndrome are living longer

E N D
Health Care for Adolescents and Adults with Down Syndrome1st India International Conference on Down SyndromeSeptember 2017 George T Capone, M.D. Kennedy Krieger Institute, Baltimore Maryland
Persons with Down syndrome are living longer Recognition of specific health conditions, treatment and prevention Health promotion to physicians, families & individuals Increasing availability & access to health care Improved opportunities for participation in health research Health care improvements have been “uneven” Limited by access to medical knowledge, resources or implementation of best practices even minimal standards Challenge of providing care to complex individuals Much to be done! Health Care for All Persons with Down Syndrome
Increased prevalence of specific medical conditions Birth anomalies and medical conditions in newborn Acquired medical conditions in children, adolescents & adults Age-related medical conditions in adults Barriers to care Diagnostic overshadowing – all is Down syndrome DS/ID - unfamiliar to primary care providers. Lack of training Presentation - unusual, atypical, or complex Complexity - multiple, co-occurring conditions - overwhelming Attitudes – access/allocation of scarce resources Need for Regular & Sustained Health Care
Adult Health Issues Vision & Hearing Heart: CHD repair, valve disease, pulmonary HTN Respiratory: pneumonias, aspiration risk, vaccinations GI: reflux, esophagitis, slow gut motility, constipation Endocrine: Thyroid, Vitamin D Bone: bone density, degenerative arthritis Does Early Detection/Treatment Improve Quality of Life?
High Impact Health Issues Chronic, Difficult to treat Weight management: diet, physical activity Sleep: obstructive apnea, disturbed sleep Mental health: depression, anxiety, behavior Does Early Detection/Treatment Improve Quality of Life?
Overweight-Obesity The prevalence of obesity (BMI>30) is (~40%) Higher than in adults with other causes of ID (~25-30%) Limited evidence about associated medical and behavioral comorbidities or the use of biomarkers to understand obesity
Chronic Obesity Associations Emotional - Mood disorder, self-esteem Fatigue - lethargy, low alertness Metabolic – hyperglycemia, hyperlipidemia Hormonal - estrogens, appetite regulating hormones Sleep apnea – worsened Physical activity – more difficult Musculoskeletal - joint pain, degenerative changes
Preventing/Treating Overweight Emphasis on healthy diet • Meal planning and access to food requires high vigilance and supervision. • Make smart choices, don’t buy it • Lead by example, get the others on board • Vending machines at day program or job site? Emphasis on structured exercise • Programed, pre-scheduled exercise plan • Walking, dancing, Wii Fit, indoor cycle, SO sports • Walk the dog • Water aerobics, swim
Risk Factors for Obesity Female – Estrogen hormones Metabolism – lower RMR, (insulin resistance) Hypothyroidism – not often the cause Sleep apnea Eating disorder, satiety signaling (leptin, resistance) Medications - OBCP, Newer antipsychotics, SSRIs Lifestyle Low activity
Obstructive Sleep Apnea • The risk for OSA is due to both upper airway anatomy and obesity. • > 90% of adults with DS may have abnormal sleep • > 60% moderate-severe OSA (AHI) >30
Obstructive Sleep Apnea • Night-time symptoms • Snoring, respiratory pauses (>10s), gasping, sitting up, jerking movements, repositioning • Not always obvious • Daytime symptoms • Fatigue (napping), loss of initiative, slowing, innattention, mood changes (irritability, internalization and social withdrawal) • Major mood symptoms (MDE), cognitive decline and a pseudo-dementia like picture • Intensification in preexisting anxiety, disruptive behaviors
Preventing/Treating Sleep Apnea Sleep position • Elevated head of bed • Reclining chair • Side-lying CPAP/BiPAP Dental-oral appliance Airway surgery
Sleep Humans – spend up to 30% of lifetime asleep Cyclic occurrence of REM and NREM sleep stages 1st half- NREM and SWS (N3) predominate 2nd half- REM and N2 predominate Critical for memory consolidation Tissue recovery and repair
Sleep and Memory Consolidation Non-REM Sleep Slow-Wave Sleep (N3) – declarative memory Reactivation of encoded daytime memories consolidates into long-term memory REM Sleep Procedural and emotional memory Stabilizes transformed memories
Hippocampus and Memory Good – physical exercise, quality sleep Bad – OSA -sleep arousals, fragmentation (reduced SWS or REM sleep), low oxygen, stress (high cortisol), inflammation?
Prefrontal Executive Dysfunction Our most Human attributes, indeed our cultural heritage depends on prefrontal cortex Planning, Organizing, Real time (Working) memory, Behavioral self regulation, Social sophistication
Major Depressive Episode & Down Syndrome Frequency - unknown (~10%) Male = Female Grief, bereavement or adjustment reaction . More common NOT the same as Major Depression NOT a linear increase with ageing - peaks at 15-25yr Prodrome of dementia? (Amyloid peptide, deposits, monoamine and cholinergic NT failure)
Hippocampus and Mood Good – physical exercise, quality sleep Bad – OSA -sleep arousals, fragmentation (reduced SWS or REM sleep), low oxygen, stress (high cortisol), inflammation?
Does Sleep Apnea Contribute to Symptoms of Anxiety Disruptive Behavior in Adults?
Anxiety, Compulsions & Disruptive Tendencies Frequency unknown (~10%); Male = Female Mood & anxiety disorders increase during-after puberty Childhood h/o ADHD, Anxiety, Repetitive movements - that morphs and intensifies Psychosocial Stressors and Biological vulnerability Functional ADL skills: usually maintained, but behavior interferes
Making the Mental Health-Sleep Connection in Adolescents & Adults Consider a Sleep Disorder and getting a Sleep Study • NEW change in mental function (depression + decline) • Minimally-responsive or treatment-resistant symptoms of depression, mood-instability or psychosis High suspicion required Sleep Apnea may not be obvious Previous T&A is not a prevention or long-term cure Obesity is often absent
Treatment Considerations Mental Health & Co-morbid Sleep Apnea SLEEP MEDICINE: Getting an overnight sleep study is difficult CPAP mask – adherence? training program Airway surgery – tonsils, UPPP ? Dental appliance, Sleep position, Weight loss MEDICATIONS: For impairing psychiatric symptoms • Mood, Anxiety - SSRI/SNRI Antidepressants • Psychotic-like disorganization - Newer Antipsychotics • Sleep initiation & maintenance – sleep medication ? • Fatigue- Modafinil