Download
1 / 45
460 likes | 784 Vues
Substance Abuse and Veterans. Supporting Veterans and Service Members: A Mental Health and Community Imperative June 28 th , 2013 Jonathan C Fellers, MD Addiction Psychiatry Fellow Portland VA Medical Center & OHSU. Outline. Definitions Neurobiology of Reward Epidemiology Common Culprits

E N D
Substance Abuse and Veterans Supporting Veterans and Service Members: A Mental Health and Community Imperative June 28th, 2013 Jonathan C Fellers, MD Addiction Psychiatry Fellow Portland VA Medical Center & OHSU
Outline • Definitions • Neurobiology of Reward • Epidemiology • Common Culprits • Alcohol • Cannabis • Opioids
Addiction • A behavioral pattern of drug use, characterized by: • overwhelming involvement with the use of a drug (compulsive use) • the securing of the supply • a high tendency to relapse after withdrawal.
Substance Abuse Substance abuse is defined as a maladaptive pattern of substance use leading to clinically significant impairment or distress as manifested by one (or more) of the following, occurring within a 12-month period: • Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home (such as repeated absences or poor work performance related to substance use; substance-related absences, suspensions, or expulsions from school; or neglect of children or household). • Recurrent substance use in situations in which it is physically hazardous (such as driving an automobile or operating a machine when impaired by substance use) • Recurrent substance-related legal problems (such as arrests for substance related disorderly conduct) • Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance (for example, arguments with spouse about consequences of intoxication and physical fights). Note: The symptoms for abuse have never met the criteria for dependence for this class of substance. According to the DSM-IV, a person can be abusing a substance or dependent on a substance but not both at the same time.
Substance Dependence Substance dependence is defined as a maladaptive pattern of substance use leading to clinically significant impairment or distress, as manifested by three (or more) of the following, occurring any time in the same 12-month period: • Tolerance, as defined by either of the following: • A need for markedly increased amounts of the substance to achieve intoxication or the desired effect • Markedly diminished effect with continued use of the same amount of the substance. • Withdrawal, as manifested by either of the following: • The characteristic withdrawal syndrome for the substance • The same (or closely related) substance is taken to relieve or avoid withdrawal symptoms. • The substance is often taken in larger amounts or over a longer period than intended. • There is a persistent desire or unsuccessful efforts to cut down or control substance use. • A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects. • Important social, occupational, or recreational activities are given up or reduced because of substance use. • The substance use is continued despite knowledge of having a persistent physical or psychological problem that is likely to have been caused or exacerbated by the substance (for example, current cocaine use despite recognition of cocaine-induced depression or continued drinking despite recognition that an ulcer was made worse by alcohol consumption).
Substance Use Disorder A maladaptive pattern of substance use leading to clinically significant impairment or distress as manifested by two (or more) of the following, occurring within a 12-month period: • Recurrent substance use resulting in a failure to fulfill major role obligations at work, school, or home • Recurrent substance use in situations in which it is physically hazardous • Continued substance use despite having persistent or recurrent social or interpersonal problems caused or exacerbated by the effects of the substance • Tolerance, as defined by either of the following: • A need for markedly increased amounts of the substance to achieve intoxication or the desired effect • Markedly diminished effect with continued use of the same amount of the substance. • Withdrawal, as manifested by either of the following: • The characteristic withdrawal syndrome for the substance • The same (or closely related) substance is taken to relieve or avoid withdrawal symptoms. • The substance is often taken in larger amounts or over a longer period than intended. • There is a persistent desire or unsuccessful efforts to cut down or control substance use. • A great deal of time is spent in activities necessary to obtain the substance, use the substance, or recover from its effects. • Important social, occupational, or recreational activities are given up or reduced because of substance use. • The substance use is continued despite knowledge of having a persistent physical or psychological problem that is likely to have been caused or exacerbated by the substance. • Craving or a strong desire or urge to use a specific substance.
Brain Stimulation • In 1953, Olds and Mills discovered that electrodes in certain areas of rat brain served as operant reinforcers: • Nucleus accumbens • Ventral tegmental area • Medial forebrain bundle • Olds, J. & Milner, P. (1954). Positive reinforcement produced by electrical stimulation of septal area and other regions of rat brain. Journal of Comparative and Physiological Psychology, 47, 419–427.
Brain Stimulation • In 1963, Heath demonstrated in humans that stimulation is pleasure producing • “During these sessions, B-19 stimulated himself to a point that he was experiencing an almost overwhelming euphoria and elation, and had to be disconnected, despite his vigorous protests" • Moan, C.E., & Heath, R. G. (1972). Septal stimulation for the initiation of heterosexual behavior in a homosexual male. Journal of Behavior Therapy and Experimental Psychiatry, 3, 23–30.
Intracranial Stimulation Medial forebrain bundle Nucleus accumbens Ventral tegmental area
Reward Circuitry • Activation of these brain areas associated with novelty, rather than pleasure • Increases the “salience” of objects • Increases the motivation to approach a gratifying object • Dopamine is the main neurotransmitter • “The final common pathway of reinforcement and reward in the brain is hypothesized to be the mesolimbic dopamine pathway”
Mesocorticolimbic Pathways Nucleus accumbens Frontal lobe Medial forebrain bundle Amygdala & hippocampus Ventral tegmental area
Epidemiology • Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (November 1, 2007). The NSDUH Report: Serious Psychological Distress and Substance Use Disorder among Veterans. Rockville, MD.
Epidemiology • Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (November 1, 2007). The NSDUH Report: Serious Psychological Distress and Substance Use Disorder among Veterans. Rockville, MD.
Epidemiology • Substance Abuse and Mental Health Services Administration, Office of Applied Studies. (November 1, 2007). The NSDUH Report: Serious Psychological Distress and Substance Use Disorder among Veterans. Rockville, MD.
Epidemiology • Bray RM, Pemberton MR, Lane ML, Hourani LL, Mattiko MJ, Babeu LA. (2010). Substance use and mental health trends among US military active duty personnel: key findings from the 2008 DoDhealth behavior survey. Mil Med. 175:6, 390.
Epidemiology • Bonn-Miller MO, Harris AHS, TraftonJA. (2012). Prevalence of cannabis use disorder diagnoses among veterans in 2002, 2008, and 2009. Psych Svs, 9(4): 404.
Epidemiology • Bray RM, Pemberton MR, Lane ML, Hourani LL, Mattiko MJ, Babeu LA. (2010). Substance use and mental health trends among US military active duty personnel: key findings from the 2008 DoDhealth behavior survey. Mil Med. 175:6, 390.
Epidemiology • Substance Abuse and Mental Health Services Administration (SAMHSA) Treatment Episode Data Set (TEDS), 2010, based on data received through October 10, 2011.
Alcohol • Most commonly abused substance • Yeast produce ethanol through the anaerobic enzymatic process • Fermentation can produce alcohol contents of up to 16%
Alcohol • Distillation can then “spirit” off alcohol to achieve up to 96% concentration (limit of ethanol-water azeotrope)
Alcohol and PTSD • The estimated prevalence of alcohol use disorders in individuals with PTSD is higher than the prevalence in the general population • In individuals with both PTSD and substance use disorders, the symptoms of PTSD tend to be more severe, particularly in the avoidance and hyperarousalclusters • There is evidence that they are more prone to substance use relapse than non co-morbid individuals • Co-morbidity of PTSD and substance use is associated with a higher rate of psychosocial and medical problems and higher utilization of inpatient hospitalization • McCarthy E, Petrakis I. (2010). Epidemiology and management of alcohol dependence in individuals with post-traumatic stress disorder. CNS Drugs. 24(12): 997-1007.
Cannabis • Several species: • Cannabis sativa • Cannabis indica • Cannabis ruderalis • Psychoactive components thought to be produced to defend the plant from predators • Most concentrated in the flowers of the female plant
Cannabis • Major psychoactive ingredient Δ9-tetrahydrocannabinol (THC) • Several other cannabinoids including cannabidiol (CBD), cannabinol (CBN), tetrahydrocannabivarin (THCV) THC CBD
Cannabis • Modern cannabis production • Selective breeding for yield and potency • Manipulation of growing conditions • Hydroponic gardening with control of light cycle, nutrients, CO2 • “Sinsemilla” technique to enhance resin production
Cannabis • Burgdorf JR, Kilmer B, & PaculaRL. (2011). Heterogeneity in the composition of marijuana seized in California. Drug Alc Dep. 117 (1), 59-61.
Medicinal Cannabinoids • Dronabinol (Marinol®) • FDA approved for treatment of anorexia in AIDS patients, and for refractory nausea and vomiting of patients undergoing chemotherapy • CN-III controlled substance THC
Medicinal Cannabinoids • Nabilone (Cesamet®) • FDA approved for treatment of chemotherapy-induced nausea and vomiting • C-II controlled substance Nabilone
Artificial Cannabinoids • Many research chemicals and analogues of THC have been created • “Legal” substitutes for cannabis: “Spice,” “K2” • Most common: cannabicyclohexanol, JWH-018 Cannabicyclohexanol JWH-018
Mechanism of Action • Endocannabinoid system • CB1 (CNS) • CB2 (periphery) • Endogenous ligands • Anandamide • 2-arachidonoyl glycerol Anandamide
Acute Effects • Mild euphoria • Relaxation • Perceptual alterations • Time distortion • Intensification of normal experiences • Increased sociability and laughter • Increase in appetite • Loss of short-term memory
Cannabis and PTSD • Links between PTSD and: • Using cannabis to cope • Severity of cannabis withdrawal • Craving • Boden MT, Babson KA, Vujanovic AA, Short NA, Bonn-Miller MO. (2013). Posttraumatic stress disorder and cannabis use characteristics among military veterans with cannabis dependence. Am J Addict. 22(3):277-84.
Cannabis and PTSD • Neumeister A et al. (2013). Elevated brain cannabinoid CB1 receptor availability in post-traumatic stress disorder: a positron emission tomography study. Mol Psychiatry. Advance online publication 14 May 2013.
Opioids • Opium poppy • Papaversomniferum • Opioid alkaloids concentrated in the sap of developing seed pods • Raw form called opium • In 2007, 93% of the world’s illicit opiates from Afghanistan • United Nations Office on Drugs and Crime. Afghanistan Opium Survey 2007.
Opioids • Major psychoactive ingredients are morphine and codeine • Several other important alkaloids including thebaine Morphine Codeine Thebaine
Medicinal Opioids • Synthetic variants of morphine and codeine
Heroin • Heroin is diacetylated morphine • Acetyl groups create highly lipophilic compound that rapidly crosses the blood-brain barrier and accumulates in the CNS Heroin
Mechanism of Action • Opioid system • μ receptor • Brain, spinal cord and intestinal tract • Analgesia, euphoria, miosis, physical dependence, respiratory depression, decreased GI motility • κ receptor • Brain, spinal cord • Analgesia, anticonvulsant effects, dissociative & delirianteffects, dysphoria, miosis • δ receptor • Brain • Analgesia, antidepressant effects, convulsant effects, physical dependence
Mechanism of Action • Endogenous ligands • Small peptide neurotransmitters • Endorphins • Bind to μ receptor • “Natural pain relievers,” “runner’s high” • Dynorphins • Bind to κreceptor • Modulators of pain response, maintain homeostasis through appetite control and circadian rhythm, weight control and regulation of body temperature • Enkephalins • Bind to δreceptor • Koneru A, Satyanarayana S, Rizwan S. (2009). Endogenous opioids: their physiological role and receptors. Global J Pharmacol. 3(3): 149-153.
Acute Effects • Euphoria • Decreased pain perception • Sedation • Nausea, vomitting • Respiratory depression • Decreased GI motility • Miosis
Opioid Withdrawal • Tolerance • After repeated opioid use, the body establishes a new homeostasis for the presence of opioids Euphoria Drug Effect Mood Dysphoria Baseline Mood
Norepinephrine Pathways Neocortex Hypothalamus Spinal cord Temporal lobe Locus coeruleus Thalamus Cerebellum
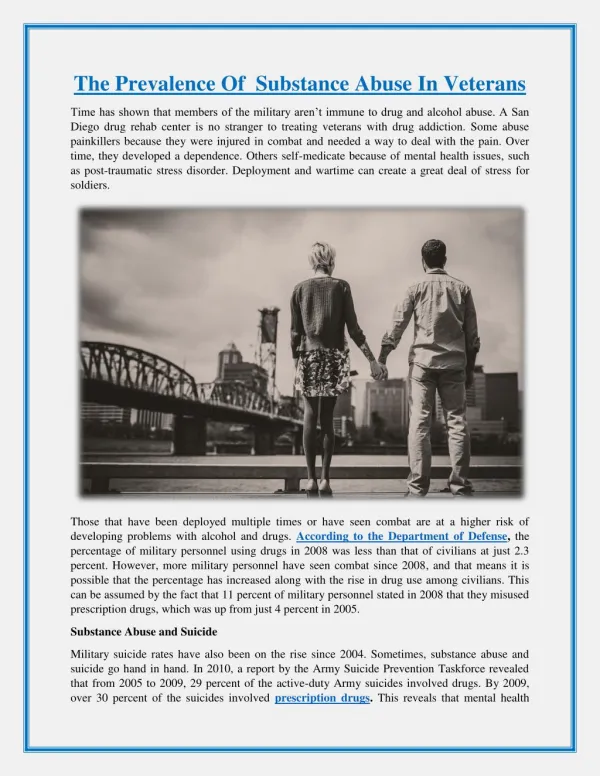
Opioids and PTSD • Use of morphine soon after injury associated with a reduced risk of PTSD (odds ratio, 0.47; p<0.001) • Among US veterans of Iraq and Afghanistan, PTSD associated with: • Prescriptions for opioids • High-risk use • Adverse clinical outcomes • Holbrook TL, Galarneau MR, Dye JL, Quinn K, Dougherty AL. (2010). Morphine use after combat injury in Iraq and post-traumatic stress disorder. N Engl J Med. 362(2): 110-7. • Seal KH, Shi Y, Cohen G, Cohen BE, Maguen S, Krebs EE, Neylan TC. (2012). Association of mental health disorders with prescription opioids and high-risk opioid use in US veterans of Iraq and Afghanistan. JAMA. 307(9): 940-7.