Download
1 / 58
600 likes | 1.66k Vues
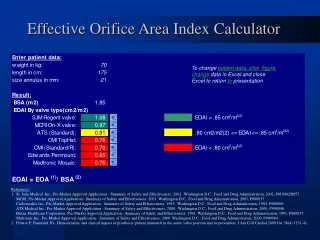
Calculation of Stenotic Valve Orifice Area. Grossman’s cardiac catheterization, angiography, and intervention. Presenter: 李政翰 Supervisor: 詹世鴻. Gorlin’s Formula. 1st hydraulic formula F=A*V*Cc ( F=flow rate, A=orifice area, V=velocity of flow, Cc=coefficient) 2nd hydraulic formula

E N D
Calculation of Stenotic Valve Orifice Area Grossman’s cardiac catheterization, angiography, and intervention Presenter:李政翰 Supervisor:詹世鴻
Gorlin’s Formula • 1st hydraulic formula F=A*V*Cc ( F=flow rate, A=orifice area, V=velocity of flow, Cc=coefficient) • 2nd hydraulic formula V2 =(Cv2)*2gh ( h=PG in cm H2O, Cv=coefficient of velocity) • A=F/(C)*44.3*h½
Gorlin’s Formula • A=F/(C)*44.3*h½ For MV or TV area calculation F=CO/(DFP*HR), C=0.85 For AV or PV area calculation F=CO/(SFP*HR), C=1
Mitral Valve Area • A=F/(C)*44.3*h½h=x(F/A)2 F=CO/(HR)(DFP) h=x[CO/(HR)(DFP)A] 2
Example of Calculation of MS • CO=4680 cm3 /min, HR=80 beats/min DFP=0.4 sec/beat MVA=0.71cm2
Pitfalls • Pulmonary Capillary Wedge Tracing Nishimura PG of MV was larger 3.3±3.5mm Hg when PAWP replaced LAP Lange Direct measure (Transseptal) LAP, PAWP was larger only 1.7± 0.6 mmHg
Pitfalls • The authors PAWP could substitute LAP except in: a. pulmonary venoocclusive disease b. cor triatriatum c. failure to wedge properly • One should verify proper wedge a. mean wedge pressure< mean PA b. PaO2 ≥95% or at least equal to artery
Pitfalls • Alignment Mismatch There is a time delay in the transmission of LA pressure. • Realignment of a wedge tracing is practically more physiologic realignment
Pitfalls • Calibration Errors • Cardiac Output determination CO should be measured simultaneously with the gradient determination MR and TR would make CO measurement inaccurate
Aortic Valve Area • Critical Stenosis ~0.7cm2 Critical abrupt worsening of prognosis • PG=x[CO/(HR)(SFP)A] 2
Aortic Valve Area • Critical Valve stenosis may be determined by body size
Example • The average PG: 40mmHg • Systolic ejection period: 0.33 sec • HR: 74 bpm • Cardiac output: 5000 cm3/min • AV area=5000*74*0.33/(44.3*400.5)=0.7cm2
Is peripheral arterial pressure a satisfactory substitute for ascending aortic pressure when measuring aortic valve gradients?
Pressure tracings recorded from two catheters within the body of the LV • If catheter tip in LVOT, it may underestimate the true LV-aorta PG up to30mmHg
PG recorded at different sites may vary widely • The differences in PG among different sites are up to45mmHg
Another approach to increasing the accuracy of transaortic valve PG
Pitfalls • Transducer calibration • Since in the absence of peripheral stenosis, mean pressure recorded by both catheters should be identical
Pitfalls • Pullback Hemodynamics • Carabello’s sign Increase in peripheral systolic pressure of more than 5 mmHg when LV catheter pullback • This sign is present in more than 80% critical AS (AV area ≤0.5cm2)
Area of TV and PV • Rare TV or PV stenosis in adults • In general, mean PG≥5mmHg across TV is sufficient to cause RV failure signs • PG≤50mmHg across PV are usually tolerated • PG≥100mmHg indicate surgical correction
Alternatives to the Gorlin Formula • Hakki (tested in 100 patients with AS or MS) Valve area=CO(l/min)/PG1/2 Ex.1 (MS,0.71cm2): MVA=4.68/301/2=0.85cm2 Ex.2 (AS,0.73cm2 ): AV area=5/401/2=0.79cm2
Assessment of AS in patients with low cardiac output • Based on Gorlin Formula, Valve area depends on cardiac output. • Two mechanisms: a. increase CO and LV pressure physically opens the valve b. incorrect empirical coefficient factor for AV
Assessment of AS in patients with low cardiac output • There are two conditions we should distinguish a. intrinsic LV dysfunction combines with mild AS b. critical AS related LV dysfunction
Valve Resistence • AV resistence= 1.33(mean PG)(SEP)(HR)/CO less flow-dependent, may be an important adjunct in patients with low CO
Recommendation of AS in patients with low cardiac output • For patients with CO≤4.5l/min, PG≤40mmHg, AV resistance≤275dyn-sec-cm-5 • Recommend Nitroprusside or dobutamine infusion test a. if PG increases probable severe AS b. if PG decreases or slightly decreases and CO increases not severe AS, unlikely benefit from AVR
Mitral Stenosis • Normal orifice: about 4.5cm2 • First, LA pressure rises and increase PG between LA and LV • Second, reduction of blood flow across MV • Third, pulmonary edema developed and reactive pulmonary arterial change • Two stenoses MV and Pul. arterioles
Catheterization Protocol • Indication: consider balloon mitral valvuloplasty or MVR • Procedure of right and left sided heart should be evaluated
Catheterization Protocol • Usual indication for MS balloon mitral valvuloplasty or corrective surgery • Both sided heart should be evaluated A. Simultaneous PAWP and LV pressure tracings for mitral orifice B. if PG between MV < 5mmHg, error is large. Induced tachycardia and increase preload should be done for increasing PG
Catheterization Protocol C. Measure PA, PAWP and cardiac output for calculating pulmonary vascular resistence. D. RV and RA for RV function E. Other valvular heart disease or congenital heart disease may co-exist
Mitral Regurgitation • Mitral valve apparatus leaflets, papillary muscles, chordae tendineae and annulus • Rheumatic heart disease, IE, MVP, AMI, LV dilatation
MR • MR severity determined by: a. regurgitant orifice b. LA compliance c. PG between LA and LV during systole d. duration of systole e. afterload of LV
Hemodynamic assessment • Both sided heart pressure evaluation • Interpretation of V wave in PAWP tracing: Prominent V waves are insensitive and poor positive predictive for identifying mod or severe MR ex. Left heart failure also had prominent V waves. Giant V waves 3x PAWP or mean LA
Exercise Hemodynamics • The patient usually fails to increase cardiac output appropriately with exercise (less than 80% of predicted) • PAWP or LA mean pressure commonly increase larger than 35mmHg by 4-5 minutes of supine bicycle exercise
Angiographic Assessment • LV angiography evaluate the severity of MR Mild (1+)clear with each beat Moderate (2+)does not clear with each beat and opacify entire LA after beats Mod-severe (3+)complete opacify and equal opacification Severe (4+) one beat opacify whole LA and stronger than LV and reflux to PV
Regurgitation Fraction • TSV (total LV stroke volume) • FSV (forward LV stroke volume) • RSV (regurgitant stroke volume) • RF (regurgilant fraction) • RF=RSV/TSV • Grade I <20% • Grade II 20-40% • Grade III 41-60% • Grade IV >60%
Catheterization Protocol • Right heart cath RA, RV, PA, PAWP (V waves height) • Left heart cath LVEDP severe MR LVEDP<<LAP or PAWP LV failure of CAD LVEDP~ LAP or PAWP AR LVEDP>> LAP or PAWP • Measure cardiac output • LV angiography for MR and LVEF • Coronary angiography • Pharmacologic intervention nitroprusside would increase cardiac output
Aortic Stenosis • Valvular, subvalvular and supravalvular • LV hypertrophy AS related • Indications for cath LV failure, angina, syncope
Hemodynamic assessment • Simultaneous measurement of pressure and flow across the AV
Carabello’s sign • LV catheter pullback in severe AS (AV area <= 0.6 cm2 ) would increase 5 mmHg in peripheral artery
Angiographic assessment • AS may result in high LVEDP intolerant to LV angiography • Aortography is usually not required except in condition when wide aortic pulse pressure • Selective coronary angiography is necessary especially if chest pain exists
Catheterization Protocol • Right heart cath for pressure and cardiac output • Left heart cath for PG, LVEDP and trasmitral PG for concurrent MS (Sones catheter/ 0.35-inch guidewire via transbrachial artery; pigtail/straight guidewire; transseptal approach) • Aortography is helpful in evaluating AS combined with AR
Aortic regurgitation • Large stroke volume produces elevated SBP and regurgitation reduces DBP • Aortic and LV pressure may equalize in diastolediastasis • AR elevated LV pressure in diastole premature closure of MV especially acute AR
Diastole diastasis between LV and FA High late LVEDP exceed LA and PAWP premature MV closure
Acute Versus Chronic AR • Widened pulse pressure chronic • Tachycardia acute • Peak systolic FA pressure may exceed central aortic pressure by 20-50 mmHg
Angiographic Accessment • 1+ cleared by each beat and never fills the ventricle • 2+ faint opacification of the entire LV • 3+ equal opacification as LV • 4+ complete, dense opacification of LV chamber in one beat and denser than ascending aorta
Catheterization Protocol • Right heart cath • Left heart cath • LV angigraphy, Aortography and selective coronary angiography • If resting hemodynamics are normal, consider stress intervention such as dynamic exercise
Tricuspid Regurgitation • Functional TR RV dilatation and failure due to pulmonary hypertension (MS, cardiomyopathy, PPH, cor pulmonale or pulmonary embolism) • Organic TR disease of valve and its apparatus due to IE, RHD or RV infarction