Innate Recognition
Innate Recognition. Dr Kathy Triantafilou University of Sussex School of Life Sciences Falmer, Brighton. Recommended books. Immunobiology by Janeway and Travers. “Immunity” Ability to fight off infection. Innate (non-specific) immunity basic resistance to disease anatomic barriers

Innate Recognition
E N D
Presentation Transcript
Innate Recognition Dr Kathy Triantafilou University of Sussex School of Life Sciences Falmer, Brighton
Recommended books • Immunobiology by Janeway and Travers
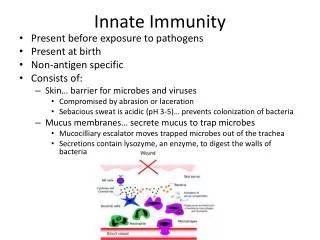
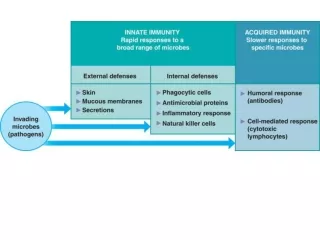
“Immunity”Ability to fight off infection • Innate (non-specific) immunity • basic resistance to disease • anatomic barriers • physiologic barriers • endocytic • phagocytic • inflammation • Acquired (specific) immunity • specificity • diversity • memory • self/non-self discrimination
Anatomic barriers • Skin • several layers of tightly packed epithelial cells • hair follicles • sweat glands • Mucous membranes (respiratory and urogenital tracks) • saliva • tears • mucous secretions
Physiologic barriers • Temperature • many species are not susceptible to certain diseases because of their body temperature (i.e. chickens and anthrax) • pH • gastric acidity • Various soluble factors • lysozyme (hydrolytic enzyme found in mucous) • interferons (produced by virus-infected cells) • complement (serum proteins that cause membrane-damaging reactions)
Endocytic barriers • Endocytosis • the macromolecules contained within the extracellular tissue fluid are internalised by the cells • internalisation occurs as small regions of the plasma membrane invaginate, or fold inward forming small emdocytic vesicles • endocytosis occurs either through pinocytosis or receptor mediated endocytosis
Inflammatory response • Inflammatory response: tissue damage caused by a wound or by invasion of a pathogenic microorganism induces a complex sequence of events • Celsus (First century A.D. Roman physician) described four cardinal signs of inflammation: • rubor (redness) • tumor (swelling) • calor (heat) • dolor (pain)
Signs of inflammation • Vasolidation • increase in the diameter of blood vessels • engorgement of the capillary network • tissue redness and increased temperature • Increased capillary permeability • influx of fluid into the tissue • Influx of phagocytic cells • migration of white blood cells and phagocytosis
Signs of inflammation • Influx of phagocytes from the capillaries into the tissue: • Margination • attachment of cells to the endothelial wall of the blood vessel • diapedesis or extravasation • emigration between the capillary-endothelial cells • chemotaxis • migration through the tissue at the site of infection
Pattern recognition receptors • Pattern recognition receptors are employed by the innate immune system in order to recognise pathogens • Pattern recognition receptors (PRRs) • receptors on lymphocytes able to recognise antigens • Antigenic arrays or patterns called pathogen-associated molecular patterns (PAMPs)
PAMPs • Pathogen-associated molecular patterns (PAMPs) are: • bacterial lipopolysaccharide (LPS) • bacterial lipoteichoic acid (LTA) • peptidoglycan • bacterial flagellin • bacterial DNA
Bacterial recognition • Recognition of bacterial components by the innate immune system can sometimes provoke a strong pro-inflammatory response • The production and release of potent pro-inflammatory mediators (such as TNF-a,IL-6, IL-1 etc) is also triggered • Uncontrollable cytokine production can result in cardiovascular collapse, hemodynamic instability and eventually cause sepsis syndrome
Septic Shock • Causes approximately 175,000 deaths annually in the U.S. • Afflicts about 500,000 Americans annually • Gram negative sepsis alone accounts for up to 1/2 of the cases (70,000-300,000 cases per year) • Annual cost for treatment is an estimated $5-10 billion
Reasons why there is a high incidence of septic shock • Increased use of cytotoxic and immunosuppressive drug therapies • Increasing frequency of invasive devices, such as intravascular catheters in clinical medicine • Increased longevity of patients prone to develop sepsis • Increase in infections caused by antibiotic-resistant organisms
Development of septicemia • Once in the bloodstream the bacteria multiply uncontrollably releasing toxins in the blood • Our immune system “senses” the presence of bacteria and attempts to eliminate them • In its attempt the immune system “over-reacts” leading to the over production of mediators • This causes damage to the walls of the blood vessels allowing blood to leak out under the skin, the person develops multi-organ failures
Types of microorganisms isolated from patients with septic shock • Gram negative bacteria, the incidence of gram negative organisms vary between 50%-80% of the cases • Gram positive bacteria, vary between 6%-24% of the cases • Fungi
Major gram negative bacteria producing infections in the U.S. • Enterobacteriaceae • Escherichia Coli (38%) • Klebsiella-Enterobacter-Serratia • Proteus-Morganella-Providencia • Citrobacter • Salmonella-Shigella • Pseudomonadaceae • Pseudomonas aeruginosa (10-15%) • Other species, Pseudomonas cepacia, Pseudomonas maltophilia • Other nonfermentative bacilli • Acinetobacter calcoaceticus • Alcaligenes faecalis
What is meningitis? • Meningitis is a disease characterised by the infection of the meninges (the membranes covering the brain and spinal cord) • This inflammation is caused by a bacterial or viral infection
Bacterial meningitis • In the United Kingdom alone an estimated 6,000 children between 1 month and 23 months will get meningitis in a given year • The mortality rates are high, with 1 in 10 cases being fatal • 15-30% of the children surviving meningitis will be left with severe handicap, such as deafness or brain injury
Common pathogens • Neisseria meningitidis (most common in the UK, accounting for more than half of the cases) • Streptococcus pneumoniae • Haemophilus influenzae
Development of meningitis • The initial step is the bacterial colonization of the throat • From the throat the bacteria enter the bloodstream • Once in the bloodstream the bacteria multiply uncontrollably resulting in septicemia before they can infect the meninges • In some cases infection in the bloodstream and the meninges develops at the same time
Septicemia • Bacteria that cause meningitis can also cause septicemia (blood poisoning) as well as meningitis • Of the 80% of cases that have meningococcal meningitis, approximately 55% have both meningitis and septicemia • Septicemia is a more serious infection with a higher mortality rate (80%)
Signs and symptoms • Patients suffering from septicemia often develop a rash, called haemorrhagic rash • It starts off as a cluster of tiny blood spots, which look like pin-pricks on the skin • These become bigger and become multiple areas of obvious bleeding under the skin, like fresh “bruises” • These “bruises” then join together to form large areas of purple skin damage
Signs and symptoms • Septicemia can develop very quickly • The patient rapidly becomes unwell: • loses interest in food and surroundings • feverish and cold, with cool feet and hands • followed by coma and sometimes death
Haemorragic rash • Early stage • Advanced stage
Development of septicemia • Once in the bloodstream the bacteria multiply uncontrollably releasing toxins in the blood • Our immune system “senses” the presence of bacteria and attempts to eliminate them • In its attempt the immune system “over-reacts” leading to the over production of mediators • This causes damage to the walls of the blood vessels allowing blood to leak out under the skin, the person develops multi-organ failures
Vaccines • Neisseria has five main Groups - A,B,C, W135 and Y • Most UK meningococcal disease is caused by groups B and C • There are combined vaccines for group A and C, that can give some protection • Effective vaccines for Group B are still some years away (which accounts for 65-70% of the cases)
Current Treatment • Antibiotics (such as Rifampin, ampicillin, penicillin, gentamycin sulfate, vancomycin) • Measures to decrease pressure within the brain • Measures to decrease the fever • Oxygen therapy if the person has problems breathing • …all measures are treating the effect and not the cause
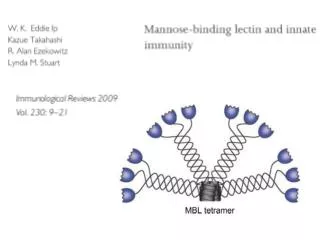
Lipopolysaccharide (LPS) • LPS is a structural component of the outer membrane of all gram-negative bacteria • pmolar concentrations are sufficient to stimulate cells of the immune, inflammatory, vascular system.
Structure of LPS • LPS consists of two chemically dissimilar domains: • The hydrophilic, polysaccharide core and O-antigen structures • A hydrophobic region known as lipid A • Virtually all LPS-induced biologic responses are lipid A dependent
(A) Schematic structure of E. Coli LPS. (B) Chemical structure of lipid A.
Molecules initially identified to be involved in the innate recognition of LPS • Lipopolysaccharide Binding Protein (LBP) (Tobias et al. 1986) • LBP, a serum protein was shown to bind LPS and transfer it to a cellular receptor • CD14 (Wright et al. 1990) • receptor for LBP-LPS complexes
LBP LPS CD14 Activation of NF-kB, MAPK, SAPK, p38
LPS Binding Protein (LBP) • A 60 kD glycoprotein (single chain polypeptide) • An acute phase reactant • Functions as an opsonin that recognises the lipid A region of LPS and forms complexes with it, and then facilitates their binding and phagocytosis by macrophages • Present at concentrations 0.5 mg/ml in the serum of healthy humans • During the acute phase it is synthesized in the hepatocytes • Reaches concentrations of 50 mg/ml in serum in the acute phase of infection
Bears NH2-terminal sequence homologous with another LPS-binding protein BPI (bactericidal/permeability-increasing protein) • BPI is stored in the specific granules of PMN and kills gram negative bacteria by binding LPS and disrupting the permeability barrier. • In contrast to BPI, LBP is not directly cytotoxic, it binds to LPS forming an LPS-LPB complex and then it attaches to cell via a receptor.
Crystal structure of BPI Beamer, et al. 1997
CD14 • Myeloid differentiation antigen expressed primarily on peripheral blood monocytes and macrophages • The CD14 gene maps to the human chromosome 5 band q23 to q31, murine chromosome 18 (a region that encodes several myeloid growth factors and receptors) • 55 kDa, glycosylphosphatidylinositol (GPI) anchored membrane protein (mCD14)
Diagram of the conserved growth factor and receptor genes located on human chromosome 5 (murine 18)
Soluble CD14 • It is also found as a soluble protein (sCD14) lacking the GPI anchor in normal blood sera, in urine, and in culture media of cells expressing it on their surface • There are two soluble forms sCD14a (48kDa), and sCD14b (56kDa)