
Patient Flow Collaborative Learning Session 4
E N D
Presentation Transcript
Patient Flow Collaborative Learning Session 4 Breakout session 1 Room M5 and M6 Alison McMillan and Prue Beams
Smoothing the path for complex medical patients Breakout session 1 Room M5 and M6 9.50 – 10.35 Rowena Clift Patient Flow Coordinator Ballarat Health Patient Flow Collaborative 5th May, 2005
Smoothing The Pathway for Complex Medical Patients
BHS and HARP Funded under 2001/2002 HARP funding round “Targeting Care Management Across the Continuum” GOAL STATEMENT To develop and enhance an effective working partnership between primary care providers and Ballarat Health Services to improve health outcomes for patients over 65 years with COPD and CHF
Aims... • To be achieved through: • Supporting people’s independence and capacity to live within the community • Increasing capacity within the health system to respond to patient needs • Clearer clinical pathways to deliver better continuity of care • Creating unity and structure between public hospitals and community care sectors
Collaborating agencies • Division of General Practice • Ballarat District Nursing & Health Care • Ballarat City Council • Ballarat Community Health Centre • Primary Care Partnerships • Ballarat Health Services
Collaboration + Cooperation = Success
Project imperatives • Reduced number of attendances of ED • Reduced number of admissions to acute medical wards • Reduced number of readmissions per episode • Improved efficiency in resource management between all health sectors • Improved consumer satisfaction • Improved health outcomes via improved management and community support
Continued... • Improved timing of intervention during acute exacerbations to reduce severity of symptoms • Improved clinical decision making based on evidence based practice • Improved access to treatment options
Target population • Over the age of 65 years • Primary diagnosis of COPD and/or CCF • Multiple attendances at ED and/or multiple emergency admission to acute hospital (ie 3 • or more admissions in 2 years) • In 2004 model trialed with Unstable Angina
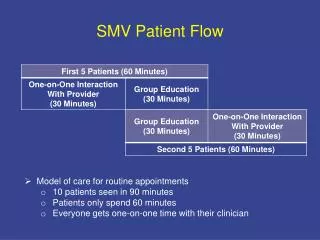
Model of Care • Preliminary multidisciplinary comprehensive • assessment in the community • Primary Physician assessment • Case Conference • - Physician • - GP • - Nursing • - Allied Health • - Community Service Providers
Model of Care Individual Care Plans for each client including: - links to community-based chronic disease self-management programs - agreed triage processes involving GP’s and/or HARP nursing staff when medical/social crises occur - 24 hour short term in-home crisis intervention - facilitated access to ED/MAP if appropriate - development of comprehensive discharge strategies on admission to acute care using individual care plans
HARP Outcomes Jan 2004 - Dec 2004Patients Managed for 6 months
HARP Outcomes July 2003 - Dec 2004 Patients Managed for 12 months or more
Outcomes Jan 04 to June 04 Interpretation of Total Score Total Score Depression Severity 1-4Minimal depression 5-9 Mild depression 10-14 Moderate depression 15-19 Moderately severe depression 20-27 Severe depression 72.7%of clients have shown a decrease in severity of symptoms 13.6%remained the same 13.6%of clients have shown an increase in severity of symptoms
Outcomes July 04 to Dec 04 QOL Measurement Interpretation of Total Score Total Score Depression Severity 1-4Minimal depression 5-9 Mild depression 10-14 Moderate depression 15-19 Moderately severe depression 20-27 Severe depression 71%of clients have shown a decrease in severity of symptoms 19%remained the same 10%of clients have shown an increase in severity of symptoms
CompOP Project – Proposed Pathway 65+ with 2 or more medical issues presenting with falls, fractures, osteoarthritis, or requiring ortho surgery, currently on ortho outpatient waiting list *Flagged medical issues Triage by Ortho CNC Contact for involvement Informed consent signed • Medical Issues • Diabetes • CCF • COPD • Cognitive disorders • Falls • Continence • Depression/Social Isolation GP engagement Assessment report to be compiled by GP including full health assessment 1. ? Further Clinic discussion required Clinic appointment made OR Case Conference Medical Specialist (who reviewed patient) Ortho Nurse, Allied Health, GP Primary in home assessment by Ortho Nurse (screening for further multidisciplinary assessment eg Physio, OT, Social Work, Dietetics) 2. Viewed by Medical Specialist GP for Ongoing review Medical Treatment Plan Individualised case management plan Appropriate Specialist Medical Clinic Eg # clinic CADAMS Health Issues Proceeds to theatre Review in Clinic Discharge Triaged by CNC Inpatient admission Discharge to GP
CompOP Objectives To develop, test and evaluate a model for collaborative complex patient care for patients, 65 years and over with orthopedic issues which: takes account of preventative, specialist and acute care options has a multidisciplinary, multi-service approach to care identifies effective options for enhanced community based care Is transferable across a range of population.
1) To reduce outpatient presentations through: • A coordinated, collaborative service provider/hospital approach to the prevention and management of complex medical issues through agreed individual service pathways (care management plans) • Availability of service coordinator to facilitate responses as appropriate • Targeting those patients with optimal potential to benefit from medical specialist outpatient clinics
2) Minimise length of stay for those requiring surgery by: • Enhancing health status on admission for those requiring surgery • The use of agreed individual service pathways to facilitate planned service provision and coordination for discharge with appropriate services and supports
3) To improve health outcomes and continuity of care processes with the development of: • Clear clinical and service pathways across the patient continuum • Single point of contact for those patients with complex medical issues • Enhanced links for those with complex conditions to appropriate self management resources and other community based programs as required • Access to specialised multidisciplinary assessment and care planning • Enhanced hospital admission and discharge processes
CompOP Outcome Measures • Decrease length of stay for target group • Decrease presentations to outpatients per patient • Decrease “Did not attends” per clinic for target group • Decrease “Not ready for care” on waiting lists for those requiring surgery • Increase in diversity of outpatient treatment options
Results to Date • The outpatients appointments list was reviewed • 404 patients were on the list • 159 medical records were audited • 56 patients were living in Ballarat with 38 patients fitting the target population • 94 patients were booked for 12 monthly review following previous Orthopaedic Surgery
Morning Tea Meet us back here for Innovations in length of stay reduction and opportunities to bundle care at 10.55
Innovations in length of stay reduction and opportunities to bundle care Breakout session 2Room M5 and M6 10.55 – 11.45 Wendy Bezzina Patient Flow Coordinator LaTrobe Regional Hospital 5th May, 2005
LOS Care Bundling Tool The LOS Care Bundling Tool presented in the “Innovations to Improve LOS Management” toolkit was used to; • Ensure the clinical process delivered key elements of care for optimal patient outcomes • Encourage clinical teams to manage unwarranted variation in care delivery • Measure compliance daily, ensuring a consistently high standard of care
Diagnostic work • The LOS Care Bundle Tool has been utilised for a period of 2 weeks prior to this presentation. • From our diagnostic work, we were able to determine we were 100% compliant at 10:30am every day, in all areas other than “Discharge by 10:30am”. • We will continue to use the LOS Care Bundle Tool going forward to assess compliance and assess the impact of other discharge planning efforts.
Constraint Area - LOS • Our average LOS in our Acute (Med/Surg) Units is historically between 3.5 - 4 days • Since the commencement of the PFC and implementation of various improvement initiatives our LOS has remained invariable. • The LOS Care Bundling Tool has clearly identified our major barrier in decreasing our LOS is Medical staff discharge practices.
Discharge Planning / Coordination Historically, we have discharged approx 8% of patients by 10:30am in our Medical and Surgical wards. Constraints to increasing this are; • Medical rounds done late in the day • No prioritisation of patient rounds • Medical Staff not flagging possible discharges • Discharge planning not appropriately prepared • Patient Transport not arriving at ‘booked’ times • NUM’s not having a clear level of responsibility for LOS, Discharge Planning and ED Admissions
Discharge Planning / Coordination - Improvement Initiatives Our Chief Medical Officer has met with Acute Medical Staff and followed up meetings with letters requesting their assistance in the following; • identifying anticipated LOS for each patient • identifying at least 2 patients per day for discharge the following day • agreement on guidelines empowering Registrars to perform discharges without Consultant review • prioritising ward rounds where patients identified for discharge, are seen at the commencement of the round
Discharge Planning / Coordination - Improvement Initiatives cont … Our Acute Medical Unit Manager has developed a ‘Unit specific’ orientation for all new Medical Staff specifically addressing; • expected admission procedures • discharge planning practices • patient transfers • pharmacy procedures One of our Acute AUM’s has recently developed a ‘Discharge Envelope’ to help patients participate in their own discharge. The envelope includes; • points detailing expected discharge time and procedure • a checklist detailing what they require prior to discharge • room inside for any information patients will take with them
Discharge Planning / Coordination - Improvement Initiatives cont … All NUM’s havebeen removed from ‘clinical’ duties and have had KRA’s developed that detail their responsibilities in relation to; • 95% Admissions from ED within 12 hours • 40% patients discharged by 10:30am daily • LOS at State Average • All KRA’s feed back into the LRH Strategic Directions, Operating Plan and Statement of Priorities and are reviewed quarterly.
Progress Positive impacts to date; • Discharges by 10:30am have increased from approx 8% to an average of 23% during the month of March. • While our average Acute LOS has remained fairly static between 3.5 - 4 days over the past 12 months, it’s hoped that improvements in Medical Staff discharge practices will see further progress.
Lessons learnt What worked well; • The Care Bundle Tool is very easy to use and only takes minutes each day to complete What would you now do differently and why? • As always, Hospital Policies need to be in place to support any changes that are being implemented.
Desired Impact Our expected impact will be; • 95% Admissions from ED within 12 hours • 40% patients discharged by 10:30am daily • LOS at State Average
Next Steps • Further work on Medical Staff discharge practices
Questions Contact: Wen Bezzina PFC Coordinator wbezzina@lrh.com.au (03) 5173 8139 ?
Lunch Meet us back here for Team tabletoppresentations at 12.45
Team presentations12.45– 3.15 • Prue Beams Room M5 and M6 • Melbourne Health • Bayside Health • LaTrobe Regional Hospital • Goulburn Valley Health • Northern Health • Metropolitan Ambulance Service
Tabletop presentations The aim of this session is to; • Promote discussion • Share “peer to peer” practical experiences of innovation • Increase energy for change and shared learning • Spread ideas between teams
Session format • 2 teams per table • Team A has 15 minutes to share experiences with team B • Whistle blows • Team B has 15 minutes to share experiences with team A • Rotation 1 • Continued…. • Working afternoon tea is available
Meet us back in the plenary for Team planning time at 3.20