Type A Behavior, Hostility, and Coronary Heart Disease: An In-Depth Review
320 likes | 435 Vues
This lecture delves into the relationship between Type A behavior, hostility, and coronary heart disease (CHD). Key studies are examined, including the Western Collaborative Group Study highlighting the incidence of CHD in Type A versus Type B individuals. The complexities of risk factors, including hostility as a potential independent risk factor, are discussed. A review of notable literature, including works by Matthews and Miller, provides an update on the current understanding of these behavioral patterns as precursors to CHD. Understanding these connections is crucial for developing effective preventive strategies.

Type A Behavior, Hostility, and Coronary Heart Disease: An In-Depth Review
E N D
Presentation Transcript
Lecture 9 Type A behaviour, hostility and CHD
Lecture 8 Reading There is material on Type A and hostility in the standard texts and general papers. See also Johnston DW 1993. The current status of the coronary prone behaviour pattern. J. Roy. Soc. Med. 86, 406-409. Dated (but short). Matthews, K 1988. Coronary heart disease and Type A behaviors: update on and alternative to the Booth-Kewley and Friedman (1987) quantitative review. Psychol. Bull. 104, 373-80. Plus reply 381-384. Interesting discussion of Type A as risk factor. Worth reading Miller et al 1991 Reasons for the trend toward null findings in research on Type A behaviour. Psychol. Bull, 110, 469-485. Serious stuff, follows up on Matthews.
Lecture 8 reading (cont.) Miller TQ et al, 1996. A meta-analytic review of research on hostility and physical health. Psychol. Bull., 119, 322-348. A comprehensive review. Best read after Matthews. Don’t get bogged down in tables.
Western Collaborative Group Study Rosenman, Brand, Jenkins, Friedman & Straus 1975 3154 men aged 30-59yrs classified on Structured Interview as either Type A or Type B Extensive measurement of other risk factors Followed up initially for 8.5 years for evidence of CHD, i.e., prospective study
Were Type A’s more likely to experience CHD? Type A Type B Number 1589 1565 No. with CHD 178 79 Incidence 13.2 5.9 (annual per 1000)
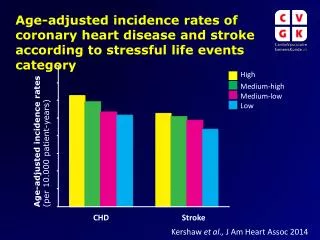
Could other risk factors explain the Type A & CHD link? Analysed using multivariate statistics but also by simpler stratified analysis. Effects still present. See incidence rates for MI (39-49) Type A Type B Non smokers 7.4 3.4 Smokers 15.4 11.4 Normotensives 7.6 1.4 Hypertensives 33.1 12.6 Low Cholesterol 5.8 2.1 High Cholesterol 20.3 11.5
When is a risk factor casual, after Everson (conference discussant) Temporality Strength of relationship Consistency Biological gradient Biological Plausibility Coherence Outcome Specificity Intervention evidence
Causality (cont) Temporality: are there prospective studies demonstrating that x precedes development of disease? Strength of relationship: How much of the variance in disease incidence explained by x? Consistency: Are studies consistent in their findings? Biological gradient: is severity and/or frequency of x associated with increasing risk of disease? Biological plausibility: what pathogenic mechanisms link x to disease?
Causality 3 Coherence: Does evidence for the relation between x and disease come from different samples (population, patient, animal models)? Outcome specificity: Is the risk associated with x exclusive to one disease? Intervention Effects: Is the disease prevented if x is treated early enough?
What happened to the WCGS later? Ragland & Brand 1988 studied survival of 257 men who had experienced CHD in original 8.5 yr follow up Ragland & Brand 1998 looked at mortality over 22 years in original sample.
Causality (cont) Temporality: are there prospective studies demonstrating that x precedes development of disease? Strength of relationship: How much of the variance in disease incidence explained by x? Consistency: Are studies consistent in their findings? Biological gradient: is severity and/or frequency of x associated with increasing risk of disease? Biological plausibility: what pathogenic mechanisms link x to disease?
Causality 3 Coherence: Does evidence for the relation between x and disease come from different samples (population, patient, animal models)? Outcome specificity: Is the risk associated with x exclusive to one disease? Intervention Effects: Is the disease prevented if x is treated early enough?
Is Type A behaviour Unitary? Many attempts to find active, toxic component Hecker et al, 1988 rated tapes of 257 men who got CHD and 257 “controls” who did not in WCGS on many attributes. Hostility significant risk factor, largely independent of Type A in this study. Relative Risk (RR) Hostility 1.92, Type A 2.68, allowing for each other Hostility 1.71, Type A 2.49. Hostility - anger or irritation involving others or hostility to interviewer. NB many now regard hostility as toxic component of Type A.
Mechanisms linking Type A or Hostility and CHD CV reactivity Effects of clotting process Other (see Kop)
Lecture 10 Depression, Vital Exhaustion and recurrent heart disease
Lecture 9 references Standard texts, Kop paper, and Krantz & Lundgren paper. Depression and CHD is very current topic and there are few good reviews. Kubzansky & Kawachi 2000. Going to the heart of the matter: do negative emotions cause coronary heart disease? J Psychosomatic Res., 48, 323-327 Review that includes depression. Carney, R M., Freedland, Miller, M (2002) Depression as a risk factor for cardiac mortality and morbidity:A review of potential mechanisms. J Psychosomatic Res., 53, 897-902. Thoughtful discussion. This is one of a number of articles on depression & health in this issue of the journal
Depression DSM-IV Five of following for at least 2 weeks Sad mood most of day, most days Loss of interest & pleasure in usual activities Sleeping difficulties Change in activity level Change in eating patterns Fatigue Negative view of self Less efficient thinking Recurrent thoughts of suicide or death
Frasure-Smith et al, 1999. Gender, depression and one-year prognosis after myocardial infarction. Psychosomatic Med. 61, 26-37. (On web through library, worth reading) Nancy Frasure-Smith major figure in proposing that depression makes reinfarction more likely. In this paper she combines her earlier studies to get large enough sample to examine effects of gender. Sample. Women 283, Men 613.
Barefoot et al, 2000 Depressive symptoms and survival of patients with coronary artery disease. Psych. Med. 62, 790-795. 1250 patients with CAD seen between 1974 & 1980 followed up for up to 19.4 years. Measure Negative Affect. 6 item covering Sad, crying, suicidal thoughts, irritability, restlessness
Vital Exhaustion (Ad Appels), see Kop Features lack of energy increased irritability demoralization Vital exhaustion is short term predictor of MI, Rotterdam Civil Servant study. 3877 healthy men followed up for 4.2 years.
Mechanisms for Depression CHD link Reactivity. Probably not Anti-depressants Other Risk factors Heart disease severity Adherence and other behavioural mechanisms Autonomic tone Blood clotting processes. PF4 and BTG increased in depressed CHD patients Inflammatory processes. Evidence of increased inflammation related to chlamydia in exhausted patients with CAD (Appels 2000)