Download

1 / 43
440 likes | 1.45k Vues
Understand the treatment algorithms for managing BPH, including pharmacological options, monitoring, and risk assessment based on patient profiles and symptoms.

E N D
BPH management. Overview of treatmentoptions Antonio Alcaraz
EAUguidelines EAU: International guidelines recommend treatment algorithms to guide medical treatment choices according to patient profile Oelke M et al. EurUrol 2013. http://dx.doi.org/10.1016/j.eururo.2013.03.004 Accessed on 8th April 2013. 2 Prescribing information can be found at the end of the presentation
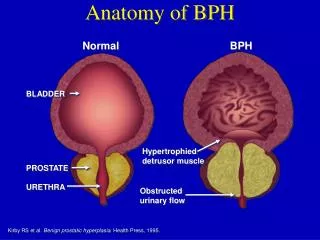
Men >40 yo Histological BPH Prostatic growth ` UT obstruction LUTS Medical therapy in BPH evolution.
BPH prevalence according definition and age Prevalence (%) 100 80 60 40 20 0 40–49 50–59 60–69 70–79 Edad (años) Pathological prevalence(n=1057) DRE(n=6975) History and physical exam(n=1057) Symptoms, IPSS (Scotland, n=699) Symptoms and flujometria (Rochester, n=2115) DRE (n=1057) Combined medical therapy in BPH
URINARY SYMPTOMS PREVALENCE IN MEN N=5460 VOIDING 25.7% FILLING 49.7% NO LUTS LUTS POST-VOIDING 16.5% 6 OUT OF10 MEN
Management options of LUTS • Prostate • Alfa blockers • Symptomatic control • 5 alfareductase inhibitors • Disease modification • Long term Symptomatic control • Surgical management • Symptomatic and modification of natural history of the disease • Bladder • Antimuscarinics • Symptomatic control
Evolution of BPH therapy. 90s • Finasteride approved in 1992 • Terasozina approved in 1993 • Doxasozina approved in 1995 • Tamsulosina approved in 1997 • Dutasteride 1998
Medical therapy and hospital admission Drug Therapy for BPH and Hospital Admission Souverein et al: Eur Urology 43:528, 2003
‘Tailor’-made treatment of BPH Drug efficacy Prostate volume PSA Sexual dysfunction Sexually active Metabolic syndrome Impacton BPH progression Risk ofside effects
EAUguidelines EAU guidelines: α-blockers/PDE5-Is should be offered to men with moderate-to-severe LUTS Storage symptoms predominant? No Prostate volume >40 ml? No Yes Long-term treatment? No Education + Lifestyle Advice with or withoutα2-blocker/PDE5-I Prostate size does not affect α1-blocker efficacy in studies with follow-up periods of <1 year but patients with a prostate volume of <40 mL seem to have better efficacy compared with those with larger glands in the longer term and is similar across age groups α1-blockers do not reduce prostate size and do not prevent AUR in long-term studies Oelke M et al. Eur Urol 2013. http://dx.doi.org/10.1016/j.eururo.2013.03.004 Accessed on 8th April 2013. Prescribing information can be found at the end of the presentation
EAU Guidelines on the Treatment and Follow-up of Non-neurogenic Male Lower Urinary Tract Symptoms Including Benign Prostatic Obstruction (BPO) * • EAU guidelines recommend alpha-1 blockers to be offered to men with moderate-to-severe LUTS based on level 1A evidence. • α1-blockers are often considered the first-line drug treatment of male LUTS because of their rapid onset of action, good efficacy, as well as the low rate and severity of adverse events. *we mentioned here the section related to Alpha-blocker only M. Oelke et al, EUROPEAN UROLOGY 6 4 ( 2 0 1 3 ) 1 1 8 – 1 4 0
a1-adrenoceptor antagonists (a1-blockers) • Efficacy • Controlled studies have shown that α1-blockers typically reduce the International Prostate Symptom Score (IPSS), after a run-in period, by approximately 30-40% and increase the maximum urinary flow rate (Qmax) by approximately 20-25%. • significant efficacy of α1-blockers over placebo was demonstrated within hours to days and maintained over at least 4 years. Alf 053 DA NE (NE) 09-13 M. Oelke et al, EUROPEAN UROLOGY 6 4 ( 2 0 1 3 ) 1 1 8 – 1 4 0
‘Tailor’-made treatment of BPH Risk ofside effects
AUA meta-analysis: dizziness with medical therapies ALFUZOSIN Doxazosin TAMSULOSIN* Terazosin FINASTERIDE Alfuzosin/Finasteride Doxazosin/Finasteride Terazosin/Finasteride PLACEBO 0% 10% 20% 30% Estimated Occurrence Rate with 95% CI *Tamsulosin 0.4mg to 0.8mg AUA Guidelines on Management of BPH J. Urol. 2003, 170, 530-547
AUA meta-analysis: symptomatic postural hypotension ALFUZOSIN Doxazosin TAMSULOSIN* Terazosin FINASTERIDE Alfuzosin/Finasteride Doxazosin/Finasteride Terazosin/Finasteride PLACEBO 0% 10% 20% 30% Estimated Occurrence Rate with 95% CI *Tamsulosin 0.4mg to 0.8mg AUA Guidelines on Management of BPH J. Urol. 2003, 170, 530-547
AUA meta-analysis: headache with medical therapies ALFUZOSIN Doxazosin TAMSULOSIN* Terazosin FINASTERIDE Alfuzosin/Finasteride Doxazosin/Finasteride Terazosin/Finasteride PLACEBO 0% 10% 20% 30% Estimated Occurrence Rate with 95% CI *Tamsulosin 0.4mg to 0.8mg AUA Guidelines on Management of BPH J. Urol. 2003, 170, 530-547
ALFUZOSIN Doxazosin TAMSULOSIN Terazosin FINASTERIDE Alfuzosin/Finasteride Doxazosin/Finasteride Terazosin/Finasteride PLACEBO Estimated Occurrence Rate with 95% CI 0% 10% 20% 30% AUA meta-analysis: ejaculatory dysfunction with medical therapies AUA Guidelines on Management of BPH J. Urol. 2003, 170, 530-547
‘Tailor’-made treatment of BPH Sexually active Sexual dysfunction Co-prescription with PDE5 inhibitors? Deleterious effects on ejaculation? Improving erection and ejaculation?
Multinational Survey of Ageing Male (MSAM-7) • Patients: • 12,815 patients representative of men 50–80 years in 7 countries (US, UK, F, Ge, I, Sp, NL) • Methods: postal questionnaire • Demographic characteristics • IPSS • DAN-PSSsex, IIEF • Co-morbidity Rosen et al. Eur Urol 2003; 44: 637- 49
MSAM-7: ED, LUTS & Age Average IIEF* LUTS Age (years) *International Index of Erectile Function (IIEF); 26 to 30 = normal erectile function; 22 to 25 = mild ED;17 to 21 = mild-to-moderate ED;11 to 16 = moderate ED; ≤10 = severe ED. Rosen R et al. Eur Urol. 2003;44:637-649
MSAM-7: Conclusions • BPH/LUTS, ED and EjD are common problems in aging men • Presence and severity of BPH/LUTS is a major, independent risk factor for sexual dysfunction • Sexual function should be considered in the initial evaluation of men with BPH/LUTS Rosen et al. Eur Urol 2003; 44: 637-49
Is ejaculatory dysfunction (EjD)observed with tamsulosindue to retrogradeejaculation?
ABEJAC study Change in ejaculate volume Change in urine sperm concentration p=ns *Tam vs Pbo, p<0.001 Tam vs Alf, p<0.001 +1.7 +0.4 +0.3 +1.4 +1.2 -2.4 * Mean ±sd value at baseline 48 ± 0.5 million/ml Mean ±sd value at baseline 3.4 ± 1.4 ml Tamsulosin 0.8mg OD Alfuzosin 10mg OD Placebo Intent to treat population Hellstrom W. J. Urol. 2006, 176, 1529-1533
ABEJAC Study Complete unejaculation 35.4% Percentage of patients 0% 0% Tamsulosin 0.8mg OD Alfuzosin 10mg OD Placebo Among completers (n=48) Hellstrom,WJG. J Urol. 2006, 176, 1529-33
EAUguidelines EAU guidelines: α-blockers/PDE5-Is should be offered to men with moderate-to-severe LUTS Storage symptoms predominant? No Prostate volume >40 ml? No Yes Long-term treatment? No Education + Lifestyle Advice with or withoutα2-blocker/PDE5-I Prostate size does not affect α1-blocker efficacy in studies with follow-up periods of <1 year but patients with a prostate volume of <40 mL seem to have better efficacy compared with those with larger glands in the longer term and is similar across age groups α1-blockers do not reduce prostate size and do not prevent AUR in long-term studies Oelke M et al. Eur Urol 2013. http://dx.doi.org/10.1016/j.eururo.2013.03.004 Accessed on 8th April 2013. Prescribing information can be found at the end of the presentation
Background • LUTS and sexual dysfunction are strongly associated1-2 • The co-prescription of drugs treating LUTS and ED is increasing • Both PDE5 inhibitors and α1-blockers may have an impact on blood pressure which differs from one drug to another in a same class 1Rosen et al. Eur.Urol. 2003; 44: 637-649 2Vallancien et al. J.Urol. 2003; 169: 2257-2261
PDE5i and BPH Egerdie RB et al. J Sex MDE 2012;9:271–281 Porst et al. EurUrol2011;60(5):1105-13. Roehrborn et al. J Urol 2008;180(4):1228-34. Oelke M et al. Eur Urol 2012;61: 917- 925
ConfirmatorystudyTadalafil 5 mg: Cambio mDEio mínimo en el IPSS total ** * ** Basal Semana 1a Semana 4 Semana 8 Semana 12 *p<0,05, **p<0,01, Porst et al. Eur Urol 2011;60(5):1105-13.
Tadalafil: 12 monthseffect IPSS per visit1,2 IPSS total media Change at theend of thetreatment (UOR, n = 416)mean (DS) Placebo → 5 mg -2,2 (5,3) 0,2 (5,4) 5 mg → 5 mg Periodo doble ciego controladocon placebo Extensión abierta con Tadalafilo 5 mg diario Semana 8 10 11 3 9 12 Visita 6 Thelongtreatmentwithtadalafilo 5mg dailywereeffective in maintainthereduction of LUTS/BPH. This trial of 12 monthswastheampliation of thestudylookingfor doses. Donatucci et al. BJU Int 2011;107(7):1110-6.
Interaction Studies • 3 placebo-controlled, randomized, cross-over studies assessed the hemodynamic interactionof Tadalafil 20mg with α1-blockers: • Doxazosin 0.8mg (18 healthy volunteers)1 • Tamsulosin 0.4mg (18 healthy volunteers)1 • Alfuzosin 10mg OD (18 healthy volunteers)2 • Endpoints: • Maximal post-baseline drop in standing and supine SBP and DBP (primary) • Outliers (secondary): SBP<85 mmHg, DBP<45 mmHg, drop in SBP vs baseline >30 mmHg, drop in DBP vs baseline >20 mmHg 1Kloner RA et al. J Urol. 2004;172:1935-19402Giuliano F. et al. Urology 2006 67, 1199-1204 .
Difference vs Placebo in Maximum Dropin Supine & Standing Blood Pressure Supine Standing SBP DBP DBP SBP * * * *statistically significant(95% CI did not contain 0) * 1Kloner RA et al. J Urol. 2004;172:1935-19402Giuliano F. et al. Urology 2006 67, 1199-1204 .
Conclusions • Tadalafil augments the hypotensive effect of doxazosin but shows marginal hemodynamic interaction with alfuzosin and tamsulosin
EAUguidelines EAU guidelines: α-blockers/PDE5-Isshould be offered to men with moderate-to-severe LUTS Storage symptoms predominant? No Prostate volume >40 ml? No Yes Long-term treatment? No Education + Lifestyle Advice with or withoutα2-blocker/PDE5-I Prostatesizedoesnotaffect α1-blocker efficacy in studies with follow-up periods of <1 year but patients with a prostate volume of <40 mL seem to have better efficacy compared with those with larger glands in the longer term and is similar across age groups α1-blockers do not reduce prostate size and do not prevent AUR in long-termstudies Oelke M et al. Eur Urol 2013. http://dx.doi.org/10.1016/j.eururo.2013.03.004 Accessed on 8th April 2013.
2000s. MTOPS study (Medical Therapy of Prostatic Symptoms) 3047 PATIENTS Finasteride 5mg Doxazosin 4-8mg Combined therapy Placebo Follow-up: 4.5 years Age >50 IPSS 8-30 Q max 8-15 ml/sec No requirements of prostate volume No requirements regarding minimum PSA McConnell JD, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of BPH. N Engl J Med. 2003;349:2387.
MTOPS – invasive therapy needed Placebo Doxazosin (p=ns) Finasteride (p<0.001) Combo (p<0.001) Incidence (%) 10 8 6 4 2 0 0.0 0.5 1.0 1.5 2.0 2.5 3.0 3.5 4.0 4.5 5.0 5.5 Años McConnell JD, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of BPH. N Engl J Med. 2003;349:2387. McConnell et al. NEJM 2003
MTOPS – Accumulatedindex of progression 67% McConnell JD, et al. The long-term effect of doxazosin, finasteride, and combination therapy on the clinical progression of BPH. N Engl J Med. 2003;349:2387. McConnell JD, et al. MTOPS. N Engl J Med. 2003
High prostate volume, PSA. High PVR and low Qmax • Marked intravesical protrusion. • Deterioration with medical therapy.