Download
1 / 22
220 likes | 247 Vues
M Rice, V Valeanu , I Delikonstantinou , E Wilson, A Orlando. 2017/2018 Sentinel Lymph Node Biopsy in Malignant Melanoma. SLNB Surgical Protocol. 1 Pre-op lymphoscintigraphy with radio colloid. 2 Dermal injection with patent blue. 3 WLE of MM scar.

E N D
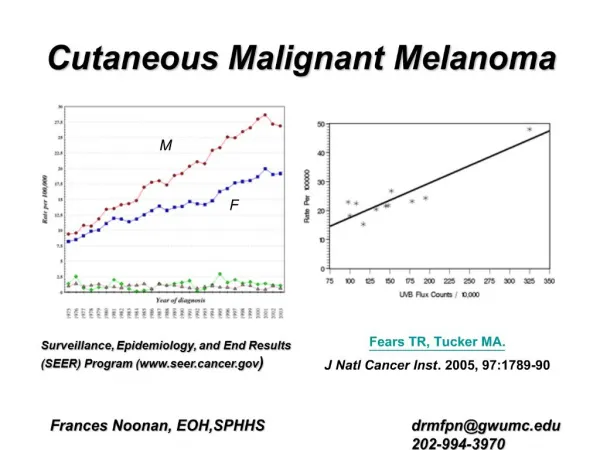
M Rice, V Valeanu, I Delikonstantinou, E Wilson, A Orlando 2017/2018Sentinel Lymph Node Biopsy in Malignant Melanoma
SLNB Surgical Protocol 1 Pre-op lymphoscintigraphy with radio colloid 2 Dermal injection with patent blue 3 WLE of MM scar 4 Gamma probe guided SLNB (>95% accuracy when performed with dermal injection)
Why Perform SLNB? • A Staging Procedure • Key prognostic indicator in Melanoma and determinant of access to adjuvant therapy • NICE (2015): indicate SLNB in Stage 1B with Breslow >1.0mm • AJCC 8th edition : 0.8mm Breslow or ulcerating lesion • Melanoma Focus Group 2019: pT1b, particularly when: a. Lymphovascular invasion b. Mitotic rate ≥2/mm2
Aims • Continue Annual Audit of SLNB @ NBT • Measure Surgical Outcomes of SLNB @ NBT • Compare practice against NICE guidance Cycle 1 July 2014 – June 2016 Cycle 2 July 2016 – June 2017 Cycle 3 July 2017 – June 2018
Methods • Retrospective review of Medical Records: • Demographics • Timings • Histopathology reports • Outcomes • Patients coding for Melanoma identified from Business Intelligence Services • Electronic notes, Discharge Summaries and ICE reports reviewed • Compare to previous data and guidelines
Results: Case Load 99 90 85 50 Increase in patients seen since last year – 10% Increase in SLNB procedures since last year – 14%
Female • 30.9% 99 Patient identified in 2017 – 2018 Male to Female: 1.41 / 1 • Male • 69.1% Gender Distribution 2014-2016 Gender Distribution 2016-2017 Results: Gender Distribution Male 52.2% Female 47.8% 2015-16 85 patients 2014-15 50 patients • Female • 41% • Male • 59% 90 patients
Results: Age Distribution Average: 64 yrs Median: 60 yrs Average: 59.7 yrs (prev 58.7) Median: 60 yrs Age Distribution 2016-17
Referral Geography 2016/17 Results: Melanoma Referral Geography Referral by Geography 21 15 18
Results: Diagnosis of Primary Lesion • Mainly GPs 4/5 • Reflection education • 3 GPs
Results: Time Targets SWAG Network Skin Cancer SSG Meeting Sept 2017 http://www.swscn.org.uk/wp/wp-content/uploads/2014/11/ https://www.england.nhs.uk/statistics/wp-content/uploads/sites/2/2017/06/Cancer-Waiting-Times-Annual-Report-201617-1.pdf SWAG_Skin_SSG_Draft_Notes_13092017.pdf
Results: Breslow Thickness Average BT = 2.54 (2.18) Average BT SLNB -VE = 2.43 (2.04) Average BT SLNB +VE = 2.72 (2.17)
Results: Primary MM Site 2016/17 26 4 18
Results: WLE Margins • NCCN Clinical Practice Guidelines in Oncology (NCCN Guidelines): Melanoma, version 1.2013. National Comprehensive Cancer Network; Fort Washington, PA: 2013. www.NCCN.org • NICE Melanoma: assessment and management (NG14) . July 2015 https://www.nice.org.uk/guidance/ng14
Results: Sentinel Node Basins 7.6% 54.8% 2.9% 34.6%
Results: Sentinel Node Biopsy Status 2017-18 CLND = 22 Performed* 7 declined 1 died 2016-17 CLND = 14 Performed 4 declined * 22 Dissections performed – 2 on different sites of same patient
Results: Complications 2016-17 2016/17 SLNB Complication : 14 cases (17.2%) 2016/17 CLND Complications : 4/11 (36%) 2017-18 2017/18 SLNB Complication : 14 cases (13.7%) 2017/18 CLND Complications : 8/22 (36%) https://www.gov.uk/government/uploads/system/uploads/attachment_data/file/666465/SSI_annual_report_NHS_hospitals_2016-17.pdf https://www.nice.org.uk/guidance/cg74/resources/surveillance-report-2017-surgical-site-infections-prevention-and-treatment-2008-nice-guideline-cg74-pdf-5649242244037
Results: Complications • SLNB complications most often occurred in the Groin: 64% - Seroma or Infected Seroma • Completion Dissection complications were most common following Groin Dissection: 50% - Seroma or Infected Seroma
Conclusions • Increase in Overall Case Load (99 vs 85 patients) • Most referrals are from Dermatology and from Gloucester / Cheltenham region • Less Shave Biopsies performed (3% vs 6.6%) • Problem with meeting service time target – reduced surgical capacity for a period, higher number of metastatic cases requiring more complex procedures, reduced surgical team for a period • 14% increase in SLNB procedures performed (97 vs 81) • 36.4% increase in number of lymph node dissections undertaken (22 vs 14) • SLNB Complication rate decreased for 2nd consecutive cycle (13.7% vs 17.2%) • Dissection Complication rate remained the same (36%) – however zero mortality, no major complications, and several unusual complications unlikely to recur
Recommendations • Focus on improving hit rate regarding service time targets – increased surgical capacity and back to a full team. • Be aware of steadily increasing case load year-on-year and account of this in planning future provision