2011.03.26 Clinicopathological conference
230 likes | 488 Vues
2011.03.26 Clinicopathological conference. 指導醫師 : 婦產科 賴瓊慧醫師 趙安琪醫師 一般外科 陳訓徹醫師 腫瘤科 張獻崑醫師 影像診斷科 許銘益醫師 放射治療科 黃意婷醫師 病理科 翁世樺醫師 Moderator: 孫建峰主任. 醫學六 彭佳惠 張家華. Medical History. General Data Chart number : 2371XXX 40-year-old female

2011.03.26 Clinicopathological conference
E N D
Presentation Transcript
2011.03.26Clinicopathological conference 指導醫師: 婦產科 賴瓊慧醫師 趙安琪醫師 一般外科 陳訓徹醫師 腫瘤科 張獻崑醫師 影像診斷科 許銘益醫師 放射治療科 黃意婷醫師 病理科 翁世樺醫師 Moderator: 孫建峰主任
醫學六 彭佳惠 張家華 Medical History
General Data • Chart number : 2371XXX • 40-year-old female • Occupation: Housekeeper (previous worker) • Marriage status: married Chief Complaint (2010/7/16) Vaginal spotting for more than one month with foul odor
Present illness • LMP: 2010/06/04, denied dysmenorrhea • Prolonged vaginal spotting with foul odor for over one month • Right lower quadrant tightness with contraction sensation • No fever or chills • Right flank pain • Medication in vain • Echo showed endometrial thickness 38.4 mm • Right adnexal cyst (64*40 mm) and myoma (55 mm)
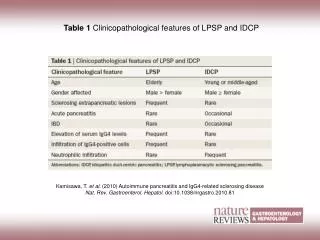
Past history • 2007/11 • Left breast cancer, s/p left partial mastectomy and dissection of axillary lymphatics • Grade III invasive ductal carcinoma, stage IIA (T1cN1Mo) with PR (3+), ER (3+) and Her-2 (1+) • 2007/12~2008/07 Breast adjuvant therapies • Chemotherapy : Epirubicin, 5-FU, and cyclophosphamide (FE90C) x 4 cycles Taxotere+CDDP x 4 cycles • Radiotherapy (2008/6~2008/7) • Tamoxifen (20mg/day) since 2008/6/3
Past history • 2009/9 • Transcervical resection (TCR) of submucosal myomectomy
Obstetric history • G7P1A6, cesarean section once 16 years ago Personal history • No known food or drug allergy. • No hypertension or DM. • Smoking: 1/2 pack per day for 15 years • HBV carrier
Family history • Father: Cardiovascular disease • Mother: not contributory • Siblings: not contributory • Cousin: Hepatocellular carcinoma
Physical Examination (2010/7/16) • BH: 156.2 cm; BW: 67.7kg; BMI: 27.7 • Fair looking; Conscious clear, E 4 V 5 M 6 • HEENT: Sclera: not icteric Conjunctiva: not paleCHEST: Bilateral clear and symmetric breathing sound HEART: Regular heart beat without audible murmur No audible S3; No audible S4
ABDOMEN: Soft and mild obese No shifting dullnessRLQ abdominal tenderness with radiation to right flank No rebounding pain or muscle guarding Bowel sound: normoactive • BACK: Knocking pain over right flank area • EXTREMITIES: No joint deformity; Freely movable; No pitting edema • SKIN: intact
Pelvic Examination (2010/7/16) • Cervix: smooth • Uterus: enlarged to 18th wk of gestational age • Vagina: smooth, dirty bloody discharge and foul smell • Adnexa: hard to be examined • Positive lifting pain of the uterus • Pregnancy test: negative
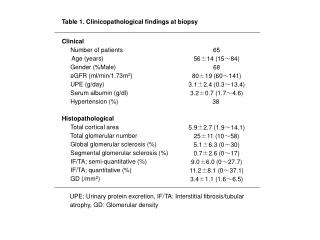
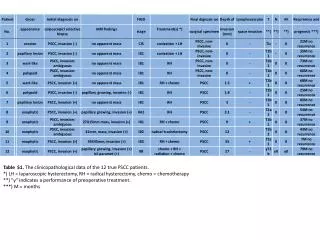
Course and Treatment • Dilatation and curettage (D&C): malignant tumor favoring adenosarcoma with sarcomatous overgrowth • Oncology survey • CT scan: A pedunculated polypoid tumor (83 mm) invaginated to fundal portion in the cavity Pelvic LN(-), PALN(-), Liver(-), Lung(-) • Bone PET: No bony metastasis • Tamoxifen held (Tamoxifen use: 2008/6/3~2010/8/2)
2010/8/6 Staging laparotomy • Total abdominal hysterectomy+bilateral salpingo-oophorectomy+pelvic lymphadenectomy+ paraaortic lymph node dissection+ partial omentectomy + appendectomy • High grade uterine adenosarcoma with sarcomatous overgrowth, invading to less than 25% of the myometrium. Cervix (-), vagina (-), bil.adnexa (-), omentum (-), pelvic LN (0/9)+ PALN(0/5), resection margin (-) FIGO Stage Ib (T1bN0M0)
2010/8~2010/12 • Adjuvant chemotherapy for EM adenosarcoma : • cisplatin + ifosfamide alternative with • doxorubicin + ifosfamide, totally 6 courses • Adjuvant endocrine therapy for breast cancer changed to aromatase inhibitor since 2010/8.
2011/1/13 • Emergency room (ER): severe lower abdominal pain KUB: no specific findings • 2011/1/20 • GYN OPD: unremarkable PV+PR: no palpable mass; atrophic vaginitis. Adhesion ileus was suspected. • Medical oncology OPD: unremarkable
2011/02/13 • ER: severe abdominal pain and chills. Palpable right upper abdominal mass • CT scan: a heterogeneous 15*15*10 cm abdominal tumor with peritoneal seeding and ascites • CA-125 : 80.4 U/mL (12/17: 8.9) • PET scan: increased uptake in abdominal area and left supraclavicular area. • Fine needle aspiration cytology of L’t neck: negative
2011/2/18 Surgery • Tumor resection with palliative right hemicolectomy and omentectomy • Op finding: One large tumor (20*18*15cm) and fragile tumors diffusely adhered with abdominal wall, small intestine and colon. Multiple small nodules scattered over mesentery and omentum. Superior mesenteric vein was encased by the tumor. Residual tumor 4 cm at SMV root.
Post-op adjuvant treatment Chemotherapy : Darcabazine (DTIC) + ifosfamide on 3/1 Radiotherapy : Intensity-modulated radiotherapy (IMRT) to the residual tumor over SMV root. Total dose: 3500 cGy/14 fx (3/7~3/25)
2011/3/15 RTO clinics: Complained of poor appetite with persistent nausea and vomiting, lower abdominal pain and distension. PE revealed a firm mass over lower abdomen. CT simulation on 3/16 showed a heterogeneous mass with more than 15x15x10 cm in size occupying the right lower abdomen and pelvic cavity Re-growing of EM sarcoma within post-op one month Palliative RT to the right lower abdomen and pelvic mass for 1900 cGy/7 fx (3/17~3/25)
2007/12-2008/7 Breast adjuvant therapies • Chemotherapy: • FE90C x4 Taxotere/CDDPx4 • RT • -HT: tamoxifen since 2008/6/3 2009/9 TCR-myomectomy : leiomyoma • 2007/11 38 y/o • Left breast cancer, T1cN1M0, s/p BCS • Pathology: • Invasive ductal carcinoma, Gr.III • LN(1/19)+, ER (3+), PR (3+), Her-2 (1+) 2/18 -Partial tumor resection -Palliative right hemicolectomy and omentectomy -Residual tumor over SMV root 2/13 ER -CT: heterogeneous 15*15*10cm abdominal tumor with peritoneal seeding and ascites. - CA-125 : 80.4 U/mL 2010/8-12 Adjuvant therapies -Chemotherapy 6 cycles -Breast endocrine therapy--> change to aromatase inhibitor • 2011/3 Adjuvant treatment • 3/1 chemotherapy • 3/7IMRT to residual tumor 8/06Staging Laparotomy - adenosarcoma with sarcomatous overgrowth, stage Ib (T1bN0M0) • 2010/7/20D&C: malignant tumor • adenosarcoma with sarcomatous • overgrowth 3/16 CT: re-growing of tumor 3/17 RT to the re-growing tumor for decompression 2011/1 ER -KUB: no specific finding 2010/8Hold Tamoxifen Staging laparotomy TCR-myomectomy Mastectomy Tamoxifen 26 months GYN F/U Palliative surgery GYN F/U 6/3 8/2 2008 2009 2010 2011 2007 9/28 2/18 10/9 11/25 10/29 8/6