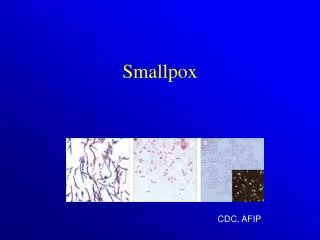
SMALLPOX
SMALLPOX. Terrorism & Science What Do We Know What Should We Do Values, Choice, Public Health and Public Policy. Grand Rounds Cambridge Hospital. William J. Bicknell, MD, MPH School of Public Health Boston University. Let’s start with a clinical look. Remember. Bottom Line.

SMALLPOX
E N D
Presentation Transcript
SMALLPOX Terrorism & Science What Do We Know What Should We Do Values, Choice, Public Health and Public Policy Grand Rounds Cambridge Hospital William J. Bicknell, MD, MPH School of Public Health Boston University
Remember Bottom Line Days 0, 1 and 2 missed Day 3 maybe Day 4 probably DaY 5 Almost for sure 3 unrecognized infectious days for sure Maybe 4 or 5 Day Zero In the mouth and throat. You don’t see it. And, very infectious Confirmation - Add 12 to 24 hours Begin vaccinating - Add 1 to 3 days Earliest Vaccination 5 days after the first case is infectious
Context & The US Issues • The Risk of Attack? • If an attack, the magnitude? • If an attack, can ring containment & quarantine work? • Vaccine risks? • Liability issues? • Are there responsible alternative options? • Who should decide what?
Today • Facts • Myths and controversies • What the US is doing • Where it was just after 911 • Where it is today • Q & A
Off the Wall? • Dr. Fenner: No errors and “A good case, reasonable for America” • Dr. Fauci: With regard to the US “….excellent and hopefully will generate some frank and needed discussion. The stepwise approach that you recommend makes sense and is quite reasonable….”
Challenges • Very limited current knowledge & experience about smallpox • No one has epidemic control in a non-immune population experience • Relevance of lessons from eradication experience (characterized by very different circumstances) is likely to be more limited than realized
The Risk of Attack • What was our estimate of 9/11 on 9/10? • I have never heard any informed person state with confidence that smallpox has not been disseminated outside the two repositories • There are reports of vaccination of N.Korean and Iraqi troops • US, UK, Israel, Germany & Australia and perhaps others are acquiring vaccine. • Israelis vaccinating first responders • The US has enough for vaccine for all residents • US is vaccinating first responders (more later) • Bottom line - Unknown but non-trivial risk of terrorist attack • Therefore, we need to know something about smallpox, let’s get some basics
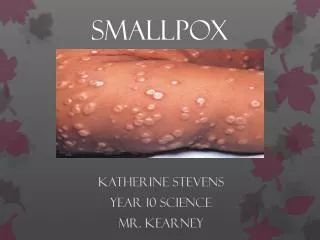
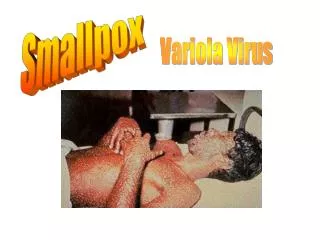
Smallpox Disease • Highly Infectious • It is dangerous and in error to say or believe otherwise • Mortality5% to > 50% - usually ~25% • 60% - 80% of survivors disfigured • Highest in young children • No specific treatment • ~ 50% of US and most populations not immune • ~ 50% may have some residual immunity • How much immunity ? No one really knows • An historical note: The Aztecs & Incas, immunologically & genetically naïve, lost to smallpox not the Spanish & Portuguese* *F. Fenner 10/11/02
Smallpox Transmission 1 • Incubation - not infectious 10 -12 days • Last days of incubation you feel lousy with Fever • Then fever drops and you feel better but not well and are infectious • Usually no visible rash yet - just inside mouth and throat • Classic rash still 2 to 4 days away • Message - Highly infectious, not very visible or obvious and not necessarily very sick • Remember terrorists are motivated folks and can be expected to walk and disseminate even though feeling ill
Smallpox transmission 2 • Close contacts are “best” - within 6 feet • Think of the morning metro or many other places • How easy is it to transmit? • Let’s consider some historical examples
A Chilling Scenario • “One person with smallpox arriving in the country traveled by train….he was apparently in the initial phase of the disease, as nobody noticed a rash on his face…Almost everyone who traveled with him in the compartment from Queensborough to Manchester contracted smallpox, the ticket collector...and those who traveled with him to Stalybridge in another train, something like a hundred people being infected from one single case.” • Not so different from flying in from Europe, traveling downtown by public transport and taking a train to the next city • And terrorists are very motivated, so expect them to travel even if feeling quite ill Wanklyn (1913) cited in Dixon p311
More Examples • Other documented examples • Yugoslavia 1972 “..denied (having a) rash..no evidence of skin lesions” 11 secondary cases • Tripoli 1946 “…a highly modified attack..unrecognized… gives rise to… fatal attacks ” A smuggler infects wife and child • Walking by a window and similar examples are found in the literature • Also true this is not always the case - but should we count on good luck? • Worse yet, aerosol by immune disseminators. • Experts I have spoken with feel, technically, this is very feasible and is reasonable to expect in a terrorist attack.
Possible Attack Rates in Terrorist Contacts Something between 10% & 50% may be a reasonable assumption Dixon, p310
The four day window • Evidence fromTripoli in 1946 (Dixon 12/48, 369-370) 21 non-immunes vaccinated within 5 days, all acquired smallpox, most mild, none died • Anecdotal evidence from the eradication years that the disease is less severe if vaccination within 4 days of contact • Vaccination within the window mayprevent death and perhapsmay prevent some disease • But the vaccinator has to find and vaccinate the infected persons • Contact tracing not likely to begin until 14 to 17 days after first exposure. In most situations, finding initial contacts within 4 days is impossible
A Recent Mathematical Model(Kaplan -Yale, Craft - MIT, Wein - Stanford) • Clearly demonstrates the limits and inadequacies of the CDC recommendation for ring containment.* • CDC has not yet adequately acknowledged and needs to update and change their website to reflect reality. • Also shows that, for any significant exposure, immediate mass vaccination is far superior. • Ratio of cases and deaths: Ring/Mass ~ 180/1 * Identify and vaccinate contacts then contacts of contacts in rings
A Recent Mathematical Model - Details(Kaplan -Yale, Craft - MIT, Wein - Stanford) • New York City • 1000 Persons initially infected • Compares Trace Vaccination (Ring Containment) and Immediate Mass Vaccination • Ring Containment: 324,000 cases, 97,000 deaths, control slow, epidemic still growing at 100 days • Mass Vaccination: 1,720 cases, 525 deaths, control fast, epidemic essentially over in 30 to 45 days • Also demonstrates limited value and great difficulties with quarantine and isolation of susceptibles and the asymptomatic
Ring Is Be More Myth than Reality • Kaplan, Wein & Craft - (Epidemiology in Press) • Central & West Africa eradication data recalculated. • Growing levels of population immunity fully explain the decline in new cases. • Bicknell Conversations with Lane, Margolis and Bloem • “We went into a village where there was a case and assumed everyone was a contact” • That’s local mass vaccination • Prof. Fenner - Surveillance, finding new cases, was critical. Then the response was local mass vaccination. • Conclusion: Contact tracing, isolation, quarantine and ring vaccination seems to have been more the exception than the rule.
But CDC still on 4 day window! • “If contacts can be vaccinated within 4 days of their contact with the smallpox case, they may be protected from developing the disease or may at least develop a less severe illness. Since smallpox is usually transmitted by close contact except under special circumstances (to be discussed later in this section), people with face-to-face or household contact with a smallpox case are the ones at greatest risk for developing the disease and should be prioritized for vaccination.” CDC Interim Plan, Guide B, 10/22/02!!! • In people exposed to smallpox, the vaccine can lessen the severity of or even prevent illness if given within 4 days after exposure. CDC “Facts About Smallpox” • Paucity of data. Therefore: Delphi of believers • An excellent example of DO NOT ALWAYS BELIEVE THE EXPERTS
Plausible US Scenario after 40 days(Play with the model ask wbicknel@bu.edu) • 5 terrorists each travel to 3 urban areas • 200 close contacts per city • 20% of contacts infected (40 cases/site) • 20% mortality • 5% of infected contacts travel to other cities • 1ary contacts infect 9 others, 2ary 5, 3ary 3 • Cities & Towns - 1,600 (21 by day 11) • Smallpox Cases - 114,000 • Smallpox Deaths - 22,000
Very Bad/Extreme Case ScenarioFirst 40 days • 10 terrorists each travel to 5 different urban areas • 500 close contacts per city • 40% of contacts infected (200 cases/site) • 30% mortality • 5% of infected contacts travel to other cities • 1ary contacts infect 10 others, 2ary 7, 3ary 4 • Cities & Towns - 40,000 (100 by day 11, then 1000s) • Smallpox Cases - 3,600,000 • Smallpox Deaths - 1,000,000
Ring Containment, Isolation & Quarantine • Eradication was accomplished in populations with high and growing population immunity, relatively low mobility and without malicious intent - A MAGNIFICANT ACHIEVMENT. • Terrorism today is different • Malicious intent • Low to absent immunity • Highly mobile terrorists and a more mobile population • Transmission to 2 or 3 - unrealistically low (Meltzer, et al) • The 4 day window - may not exist and not really relevant • Vaccination within the window not likely • Widespread isolation & quarantine - A near hopeless task, chaos and possible national shutdown • In brief - A plan that cannot work in a terrorist scenario and saw far less use in the eradication years than is commonly believed.
Ring Containment - Summary • Today, to the extent possible, with the first case or two, vaccinate probable contacts as soon as possible as you prepare for local or wider mass vaccination. • Consider contact tracing, isolation and quarantine ONLY if: • residual cases in an environment with high population immunity • an isolated exposure, particularly if there is high population immunity • Inadequate for a mobile population, with low to absent immunity and malicious exposure.
The Magnitude of an Attack • Plan for the worst, hope for the best • Malicious and well executed • Multiple terrorists, Multiple cities
The Vaccine • It works and works well • There is plenty for everyone in the US and will be lots more • It is has more side effects including deaths than other vaccines currently in wide use • Who dies and who has the most severe side effects? Children 9 and under (NEJM, p1202, 11/27/69. • Accidental inoculation most common kid to kid • About 80% of the serious complications and deaths (1968 data) avoided if children not vaccinated • Teen and adult deaths extremely rare (CDC, Israel & US military & 1968 data) • Semi-permeable membrane dressing prevents 95 to 99% of viral shedding (Dr. Belshe, 5/8/01 at CDC) • Atopic dermatitis tricky (avoiding children helps a lot) • Could contact lens wearers have a problem? (AAFP 10/17) • New and old vaccine probably similar complications • VIG good for many but not all complications
New Vaccines • Acambis -Replicating, not attenuated • Intended to mimic NYBH • Expect similar side effects • License on a fast track • Japanese LC16m8 - Replicating, attenuated • Fewer & less severe side effects • Still not OK for immunocompromised • Earliest, if developed 2005+ • Modified Vaccinia Ankara (MVA), Live non-replicating • Intention is OK for everyone • Earliest 2005+ • LC16m8 & MVA - Can we be really sure they will be effective in humans? How to know?
Vaccine Issues - 1 • Immunocompromised are at the highest risk of vaccine complications and of death from smallpox • Pre-exposure vaccination done with forethought provides a calm atmosphere where education and precautions can be assured • And if an attack, counseled to self isolate with selective vaccination based on well thought out criteria • Post-exposure will be in crisis with ability to protect the immunocompromised from complications greatly decreased: • Many will want to be vaccinated and not reveal their status • Our ability to identify and protect very limited when in crisis • Deaths from vaccine complications can be expected to exceed pre-exposure PLUS more smallpox deaths in the immunocompromised
Vaccine Issues - 2 • Accidental vaccination of contacts of vaccinees • Non-immunocompromised • Immunocompromised • Extremely rare • Almost exclusively in household contacts • Mostly children to children • Vaccine complications including deaths most common and most severe in children • Solution: • Pre-exposure do not immunize under age 9 • Screen with care • Use semi-permeable membrane dressings (Dr. Belshe) • Post-exposure drop to age 1 (and below if risk of exposure is high)
Vaccine Issues - 3 • 1968 data - Vaccination deaths in >15 all (2 of 14 million) would (should) be screened out today (aplastic anemia and leukemia) • If children <10 not vaccinated pre-exposure, careful screening and use of semi-permeable membrane dressing: • Severe complications and deaths should (my opinion) be at or below historical rates
Dilute Vaccine Lasts 180+ Days From Dr. Belshe ACIP CDC Presentation May 8, 2002
Bifurcated Needle or Jet Injector? • Jet is faster • Jet can be difficult to maintain • Some evidence of inadvertent disease transmission • US currently off the table • CDC is developing a new, safer jet injector • Dr. Bruce Weniger is the US expert at CDC
US Position - Fall 01 to Mid 02 • Reality - Limited Vaccine, have to prioritize • Did not say this, rather gave false assurances that Ring, etc.would work • State Health Officers silent • Substantial federal and state bad judgment • Believe public must be reassured - WRONG • Know it won’t work but don’t want to rock the boat - WRONG • Fear of Loosing federal funds • Possibly realistic and, to the extent it is true, reveals a dangerous perversity in the federal process
Who should decide in the US? • Attack risk is unknowable • Personal risk can be illuminated • Citizens make decisions about everything from participating in research protocols to deciding between vaginal delivery and C-section, angioplasty and open heart surgery on a daily basis • Smallpox vaccination is no more difficult, arguably much simpler with far lower risks than many other choices • Let the citizen decide within the framework of thoughtful pre-exposure guidelines • Unfortunately, we have seen that relying on PH professionals in the US may not be safe - more reason to let individuals decide for themselves
Why Voluntary Pre-Exposure Vaccination in the US? • Decreases consequences of an attack • May decrease likelihood of attack • Provides the best protection for the immunocompromised • Is low cost and relatively easy to do as part of ongoing care • Recognizes the limited surge capacity of US hospitals and near impossibility of quarantine • In case of attack • Makes containment & control much easier, whatever the strategy • Decreases panic and maintains order • Minimizes interruption of the nation’s normal business • Is realistic, has face validity and is easily understood by the professional and lay public • By decreasing the likelihood and severity of an attack may benefit the rest of the world • Will protect the most people at the lowest cost
Objections • The known risk exceeds the unknown risk and benefit • Our overall medical care delivery system is inequitable. Therefore pre-exposure vaccination will unfairly protect those with health insurance • We cannot solve all social problems before protecting against terrorism • Wait for newer safer vaccines and/or better, simpler diagnostic methods • The country needs protection today. We must plan for and use tools we have while developing better tools • We can’t vaccinate unless we are prepared to vaccinate the rest of the world • US vaccination, to the extent it decreases the likelihood of our being attacked , deceases risk to other countries. Many other countries have or are acquiring vaccine. This is fundamentally a foreign policy and foreign assistance question • A rational terrorist won’t use smallpox as it will boomerang. Let’s hope this is correct. However, it is irrational to apply our logic to terrorists
Inhibit the epidemiologic pump & first protect those most at risk • First responders, at a minimum, should include ALL staff of hospitals, clinics and physicians’ offices, EMS (~ 5.5 million people) • Enough police, fire, transport, media, public health, water, power, phone to maintain core functions of civil society • An additional ~ 5 million • Total ~ 10 million • The Federal Government decides for itself - 1,000,000 doses going to the army (NYT Oct 5)
First - a Measured Trial • Resolve liability issues • Careful guidelines to protect immunocompromised • Vaccinate 500,000 first responders (We’ve already vaccinated over 11,000 civilians since 1983, plus many military in the US until ‘90, IDF until ‘96 and Israeli first responders >9,000 now) • Ramp up VIG production (Cangene) • Observe vaccine complications very carefully • Revise guidelines and approach as indicated • Repeat with 1 to 2,000,000 first responders • Observe with care and revise as indicated • Vaccinate balance of first responders
Then - Expand to the general population • VIG now widely available • Public education as to risks and benefits of vaccination taking care to honestly and carefully distinguish between very serious/very rare and not so serious and far more common complications • Informed consent • Greatly reduce complications and deaths by restricting vaccination to: • Persons older than 9 years • Persons who are not immunocompromised and do not have other disqualifying conditions • Urge vaccinees to: • Announce their intent to family, friends and co-workers • Use appropriate dressing • Possibly consider avoiding crowds
Roles & Responsibilities • CDC • Safety guidelines for pre- and post-exposure vaccination - NOT the societal or individual risk decision • Technical assistance on request • Guidelines for pre- and post-exposure state action • States • Determine risk for their state • Make state-specific plans and recommendations • Who are first responders? • Pre-exposure guidance for general public • Post-exposure planning • Individuals • Assess their own risk • Opt or decline pre-exposure vaccination
Recommendations & Conclusions • CDC guidance for • Pre-exposure vaccination • Post-exposure vaccination • State planning frameworks • CDC technical assistance (as capacity allows) • State control • Individual choice • Assessment of risk and benefit in the US should rest with those who have the risk - Citizens • Provides the most protection, at the lowest cost, with the least chaos, and recognizes that response will and must primarily be a local and state responsibility • Pre-exposure voluntary vaccination protects against a specific threat and puts prevention first. This is what public health and responsible government are all about
Likely Results of Pre-Exposure Vaccination • Based on survey data, 50% to 70% of population will opt for vaccination • Very rare serious complications and deaths • Decreased risk to the immunocompromised from vaccination and smallpox • Trained vaccinators and supplies in place in case of attack • Possible decreased likelihood of attack • Containment and control far easier in case of attack • Hospitals and the health care system not overwhelmed • Panic, disorder and the interruption of essential services and activities minimized • Known specific preventive steps taken before a terrorist attack • The public has an example of sound proactive public health
Public Trust • Whatever is done, it is vital that actions, including discussions, take place in a way that builds public trust • Inappropriate secrecy, silence or recommendations that do not make sense erode public trust • The responses of the federal government and state health departments to bioterrorism provide an opportunity to build trust and understanding of the importance of public health • Our response to smallpox and bioterrorism, if done with humility, openly and non-defensively, can be a win for everyone, protecting the public’s health and strengthening the public health system • So far, as a nation, we have done no better than a mediocre job. The pieces are in place for a good job. Will we do it?
Take Away Messages • The first cases will be missed • 4 day window – more myth than reality • Ring containment – not for terrorism and not much else • The old vaccine, calf lymph or tissue culture, is what we know works • Other vaccines not yet ready, may work, but can we be certain? • The more that is done pre-exposure, the easier it is to contain disease post-exposure • Slight but near certain risk today to avoid possible huge individual & societal risk tomorrow.