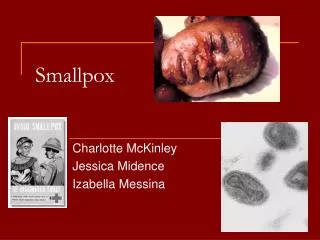
SMALLPOX
This training agenda presents an in-depth overview of smallpox pathology, epidemiology, clinical features, and prevention strategies. Participants will gain insights into the virus's transmission routes and the progression of the disease. Key topics include case definitions, differential diagnoses, symptomatology from prodrome to rash, and the critical phases of smallpox infection. Recognizing the historical context, the training emphasizes the importance of hygiene, vaccination, and public health measures that led to the eradication of smallpox in 1980, providing a thorough understanding for health professionals.

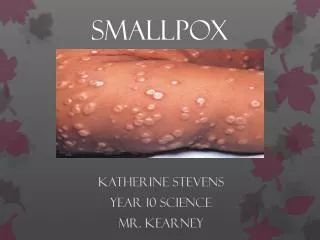
SMALLPOX
E N D
Presentation Transcript
Training Agenda • Pathogensisis • Epidemiology • Clinical Description • Case Definition • Differential Diagnoses • Pre-event evaluation for smallpox • Prevention and control • Employee health
PathogenesisJAMA, 281:2127-2137,1999, Pgs. 5-7 • Implantation of virus in oropharyngeal or respiratory mucosa • Migration and multiplication within lymph nodes • Day 3-4 after exposure asymptomatic viremia results, virus multiplies in spleen, bone marrow and lymph nodes. • Day 8, secondary viremia – fever & toxemia. Virus localizes in small blood vessels of the dermis and beneath oral and nasal mucosa.
PathogenesisJAMA, 281:2127-2137,1999, Pgs. 5-7 5. Day 12-14 – high fver, malaise, prostration, headache, backache. Sometimes severe abdominal pain and delerium. 6. Maculopapular rash appears on mucosa of mouth and pharynx, case and forearms – spreads to trunk and legs. Lesions that first appear in mouth and pharynx ulcerate release large amounts of virus into saliva. Patient most infectious up to day 7 after rash. 7. Death usually in 2nd week from toxemia associated with circulating immune complexes and soluble variola agents.
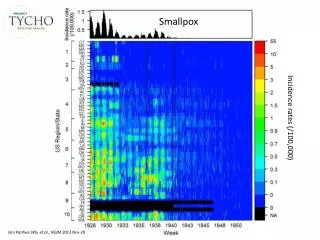
Epidemiology • 1950s: 50 million smallpox cases and an estimated 6 million deaths per year • 1960s: 15 million smallpox cases and 2 million smallpox deaths per year in 31 endemic countries • The last case of human smallpox occurred in 1977. Eradication was declared in 1980. • USA: variola major erradicated by 1926; variola minor in US by late 1940’s and in WV by 1948. †
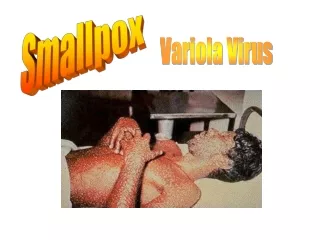
Epidemiology JAMA, 1999; 281:2127-37; CDC • Agent: variola virus • No natural reservoir • Case is BT until proven otherwise • Incubation period: 7-17 days • Person-to-person transmission: • Droplets > contact with contaminated clothing and bedding > aerosol • Mortality: 30% in pre-vaccination era • Environmental: not expected to be environmentally hardy
Environmental HardinessJAMA, 1999, 281:2127-2137, pgs 10-13 TimeTemperature(F)Humidity (%) <6 wks 87-91 80 >24 hrs 50-51 20 3 wks 95 65 8 wks 79 relatively high 12 wks 71 10
Routes of Transmission • Contacts: household members & visitors, business, travelers, & others. • Laundry – laundry workers, maids • Corpses – pathologists, morticians • Few in letters and houses of index cases
Smallpox - Progression • 7-19 days from exposure to prodrome: fever, malaise, headache, prostration, severe backache, occassional abdominal pain and vomiting • 2-4 days of fever • Fever drops • Rash onset • From rash onset: • 1-5 days: macules, papules, vesicles • 3-5 days: pustule formation • 7-21 days: scab formation • 5-14 days: death
SMALLPOX ERUPTION OVER TIME • A major diagnostic characteristic of smallpox is that lesions in a given area are similar in appearance and feel. • Progression occurs, however from area to area • Pharynx, Palate • Face • Proximal Extremities • Hands and Feet
TYPES OF SMALLPOX RASH • No rash – Variola sine eruptione • Modified • Discrete • Semi-confluent • Confluent • Flat • Hemorrhagic – early • Hemorrhagic - late
Fever 39 C Headache, backache Recovered in 48 hours Requires laboratory studies Virus isolation up to day 3 Neutralizing Antibody SMALLPOX - NO RASH VARIOLA SINE ERUPTIONE
SMALLPOX - DISCRETE Areas of normal skin between pustules even on face
SMALLPOX - SEMICONFLUENT • Pustules confluent on face but discreet elsewhere
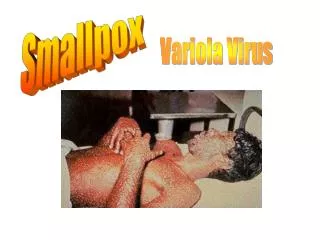
SMALLPOX - CONFLUENT • Confluent rash on face and forearms
SMALLPOX - FLAT • Pustules confluent or semiconfluent – appear flat
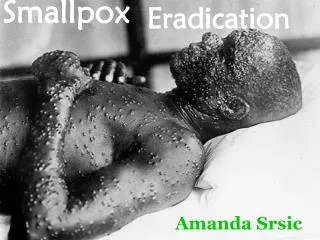
HEMORRHAGIC SMALLPOX • Widespread hemorrhage into skin • Two types (early and late) both 98% case fatality
SMALLPOX MORBIDITY BY CASE TYPE (UNVACCINATED) *Rao, Smallpox in Bombay, Kothari, Bombay, 1972 (6942 cases) Type per 100 cases
PROGRESSION OF SMALLPOX • Incubation Period • Pre-eruptive Stage • Macules • Papules • Vesicles • Pustules • Scabs • Scars
MACULES • Minute red spots (first of tongue and palate) • Lesions of the face and forehead (“herald spots”) • Proximal part of extremities • Distal parts extremities • All in 1-2 days • Very difficult to see on dark skinned people
PAPULES • Day 2 of rash • Pharyngeal lesions evolve quickly to papules, vesicles, and break down (virus present) • Raised above the skin • Fluid accumulating
VESICLES • Day 4 and 5 • Accumulation of fluid • Over next 24-48 hours, clear fluid becomes cloudy and begins to thicken
PUSTULES • Vesicles become full of pus • Most lesions pustular by day 7 • Reach their maximum size by day 11 • As fluid absorbed, lesions become flatter • Feel like hard peas in skin
UMBILICATED LESIONS PUSTULES TURNING INTO SCABS
SCABS • As fluid is absorbed scabs form • Scabs are infectious; thus patient is infectious until all scabs fall off • In areas of thick skin (palms and soles) lesions are embedded and may take 2-3 weeks to come off
COMPLICATIONS • Bacterial infection of the skin, e.g., boils, impetigo (2-5% in dirty environment); • Blood stream infection (septicemia) • Corneal ulceration and blindness: corneal opacity (4.4%), corneal ulcer (1%) • Bones and joints • Bronchitis and pneumonia probably due to secondary infection • Encephalitis: 1 in 1000 cases
SEQUELAE • Pock Marks • Scarring • Blindness • Corneal Opacities 2.1% • Blindness 0.9% • Limb Deformities • Death
Smallpox SurveillanceClinical Case Definition An illness with acute onset of fever > 101o F followed by a rash characterized by firm, deep-seated vesicles or pustules in the same stage of development without other apparent cause
Laboratory Criteria for Diagnosis of Smallpox • Isolation of smallpox virus from a clinical specimen (level D lab only) • PCR identification of Variola DNA in a clinical specimen, or • Negative stain Electron Microscopy identification of Variola virus in a clinical specimen (level D lab or approved level C lab)
Specimens for Lab Testing • Fluid from vesicles, pustules, or scabs • Autopsy specimens from major organs including skin, spleen, lymph node, liver, lung, kidney, and heart • Tonsillar tissue • Blood
Case Classification Confirmed: A case of smallpox that is lab confirmed Probable: A case that meets the clinical case definition that is not lab confirmed but is epidemiologically linked to a confirmed or probable case of smallpox
Case Classification Suspected: • A case that meets the clinical case definition but is not lab confirmed and does not have an epidemiological link to a confirmed or probable case of smallpox, OR • A case that has an atypical presentation that is not laboratory confirmed but has an epidemiological link to a confirmed or probable case of smallpox
Case Classification • Atypical presentations of smallpox • Hemorrhagic lesions • Flat, pustules remain flat, usually confluent or semi-confluent
Smallpox Outbreak • Defined as a single laboratory confirmed case
DIFFERENTIAL DIAGNOSES Chickenpox – varicella virus Other rash illnesses
MAJOR SMALLPOX CRITERIA • FEBRILE PRODROME:occurring 1-4 days before rash onset: fever >101°F and at least one of the following: prostration, headache, backache, chills, vomiting or severe abdominal pain. All smallpox patients have a febrile prodrome. The fever may drop with rash onset. • CLASSIC SMALLPOX LESIONS:deep-seated, firm/hard, round, well-circumscribed vesicles or pustules; may be umbilicated or confluent. • LESIONS IN SAME STAGE OF DEVELOPMENT:on any one part of the body (e.g., the face, or arm) all the lesions are in the same stage of development (i.e. all are vesicles, or all are pustules).
MINOR SMALLPOX CRITERIA • Centrifugal distribution: greatest concentration of lesions on face and distal extremities • First lesions on the oral mucosa/palate, face, forearms • Patient appears toxic or moribund • Slow evolution: lesions evolve from macules to papulespustules over days (each stage lasts 1-2 days) • Lesions on the palms and soles (majorityof cases)