North C-Layer Truss Ventilation Platform
10 likes | 116 Vues
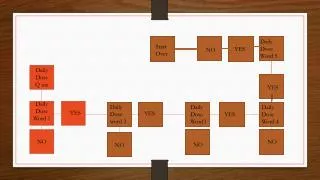
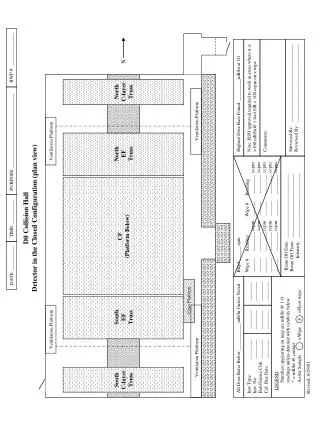
Collision hall detector in closed configuration, monitoring dose rates, wipe readings, and highest dose rate found.

North C-Layer Truss Ventilation Platform
E N D
Presentation Transcript
RWP #: ______________ N NorthC-layerTruss Ventilation Platform PURPOSE: _______________________________ Ventilation Platform NorthEFTruss D0 Collision HallDetector in the Closed Configuration (plan view) TIME: __________ CF(Platform Below) All Dose Rates Below ___________ mR/hr Unless Noted Bkgd ______ cpm Wipe # Reading Wipe # Reading______ ________ ccpm ______ ________ ccpm______ ________ ccpm ______ ________ ccpm______ ________ ccpm ______ ________ ccpm______ ________ ccpm ______ ________ ccpm______ ________ ccpm ______ ________ ccpm Highest Dose Rate Found: _________mR/hr at 1ft Inst Type: ________Inst. No: ________Batt/Source Chk: ________Cal. Due Date: ________ ________________________________ ________________________________ Note: RSO approval required to work in areas where it is>100 mR/hr@ 1 foot OR < 100 ccpm on a wipe. DATE: __________ Comments: LEGEND Numbers appearing on map are mR/hr @ 1 ft readings unless denoted with symbols below * = mR/hr @ contact A=Air Sample =Wipe =Floor wipe Beam Off Date: ___________________________ Beam Off Time: ___________________________ Intensity: ___________________________ Surveyed By: _________________________________Reviewed By: _________________________________ F Cryo Platform SouthEFTruss Ventilation Platform Ventilation Platform SouthC-layerTruss Revised: 6/29/01