Download
1 / 11
130 likes | 403 Vues
Children and HIV/AIDS. Children in Developing Countries Renata Serra – March 6 th 2007. HIV/AIDS affected children. Children may be disadvantaged or subject to discrimination when they are: HIV/AIDS Orphans: children who have lost one or both parents to AIDS Children infected by HIV

E N D
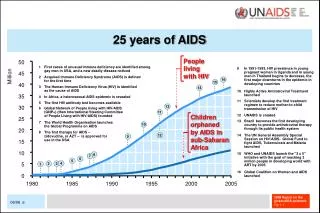
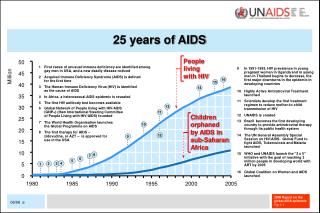
Children and HIV/AIDS Children in Developing Countries Renata Serra – March 6th 2007
HIV/AIDS affected children • Children may be disadvantaged or subject to discrimination when they are: • HIV/AIDS Orphans: children who have lost one or both parents to AIDS • Children infected by HIV • Children living in HHs where one member is HIV/AIDS • Children living in HHs which have taken up a HIV/AIDS orphan
Exposure to HIV/AIDS • Vertical transmission: mother-child • Poverty: malnutrition makes the body weak and the skin thin increasing vulnerability to HIV • Lack of family support and protection may expose children to sexual exploitation
Issues at stake • General • Emotional, material, psychological and physiological losses • Disruption of existing living arrangements • Discrimination by both children and adults • Specific • Loss of mother may mean a child is double orphan • Local ways to deal with pain and death vary • Needs differ according to child’s age/development • Adults may be differently affected and some bear disproportionate costs
Targeting • HIV/AIDS adds to other problems: poverty, lack of nutrition, exploitation, etc. • Q: Should HIV/AIDS orphans be specifically targeted? • Yes, their situation is most critical • AIDS orphans are likely to be discriminated against • The adults caring for them are already poor • No, vulnerability or poverty should be addressed instead • Some orphans do better than non-orphans, it all depends on where and with whom they live • Targeting may lead to stigmatization
Complex children’s needs • Material, emotional, psychological, relational, etc. • Young children are perceived as the most vulnerable but older children have a huge burden and need to be helped • Given individuality of needs and conditions, standardized solutions are inappropriate – hence required solutions are costly • Need to look at sibling groups rather than children individually
Community vs. institutional care • Institutional care: • Insufficient: too few resources/staff for children in needs • Segregation and dependency may result • Family and community based care • Building on own community resources • Proximity to people the child knows and loves • Extended families may not suffice, hence whole communities step in
Broadening interventions • Avoid specific targeting, involve whole communities • Devise local-specific, acceptable solutions • Make children participate • What are the best way to involve children and discuss issues with them? See “True Friends” video • Involve all community members: especially men in taking financial and other responsibilities
UN-sponsored framework for action • Strengthen the capacity of families to protect and care for OVCs • Mobilize and support community-based responses • Ensure access to essential services • Promote improved policy and legislation • Raise awareness at all levels and create a supportive environment
Current initiatives? • Comparatively little is devoted to OVCs nationally or internationally • Governments have little funds and priority are others • See example of government of Zambia • PEPFAR • 2005: $274m (out of $2.3b total budget, of which $1370m to focus countries) for care of orphans and other people affected by HIV/AIDS • Global Fund to fight AIDS, Tuberculosis and Malaria • 57% of $2b disbursed in 2005 goes to HIV/AIDS • Much less for care initiatives • Need to readdress priorities