Antiarrhythmic Drugs
890 likes | 1.98k Vues
Antiarrhythmic Drugs. Donald Blumenthal, Ph.D. Department of Pharmacology & Toxicology Don.Blumenthal@pharm.utah.edu 585-3094 Recommended Reading Goodman & Gilman Online (11th ed.), Chapt. 34 ( www.accessmedicine.com ) Harrison’s Online, Chapt 230 ( www.accessmedicine.com )

Antiarrhythmic Drugs
E N D
Presentation Transcript
Antiarrhythmic Drugs Donald Blumenthal, Ph.D. Department of Pharmacology & Toxicology Don.Blumenthal@pharm.utah.edu 585-3094 Recommended Reading Goodman & Gilman Online (11th ed.), Chapt. 34 (www.accessmedicine.com) Harrison’s Online, Chapt 230 (www.accessmedicine.com) Katzung (9th ed.), Chapt. 14, pp. 216-240 Additional Resources Used to Prepare Handout Hurst's The Heart, Manual of Cardiology On-line (11th ed.) Part 4 (www.accessmedicine.com) Clinical Pharmacology Online (Goldstandard Multimedia, www.gsm.com)
Learning Objectives • Understand the mechanistic basis, clinical usefulness, and limitations of the Vaughan-Williams classification system for antiarrhythmic drugs • Know the V-W class toxicities and other major toxicities of clinically important antiarrhythmic drugs • Know the proarrhythmic potential of specific V-W classes and drugs • Understand the importance of use-dependent blockade in antiarrhythmic drug efficacy • Know the drugs of choice for different types of arrhythmias
Arrhythmias (Dysrhythmias) • Cardiac depolarizations that deviate from normal sinus rhythm or conduction • Can be due to abnormality in one or more of the following: • Site of origin • Rate or regularity • Conduction • Cardiac arrhythmias can be benign (no symptoms), associated with mild to moderate symptoms (palpitations, syncope), or life-threatening (ventricular fibrillation, sudden death)
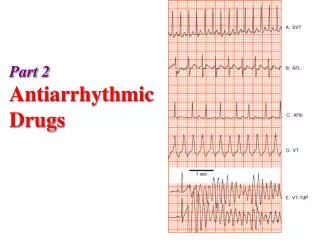
ECGs of Normal and Arrhythmic Hearts (from Goodman & Gilman)
History of Antiarrhythmic Drug Therapy • Some drugs used to treat cardiac arrhythmias have been used for hundreds of years (e.g.- quinidine and digitalis), but some have only been available for a decade or less • Research in recent years has provided much information regarding the cellular mechanisms of arrhythmias and the mechanisms by which some of the antiarrhythmic drugs act, but the general approach to antiarrhythmic therapy remains largely empirical (trial and error) • The recent results of several clinical trials, including the Cardiac Arrhythmia Suppression Trial (CAST), have indicated that many antiarrhythmic drugs may significantly increase mortality compared to placebo • Recent clinical trials, including MADIT, MADIT II, and SCD-HeFT, have indicated that ICDs can significantly decrease mortality relative to antiarrhythmic drug therapy in many patients
Cardiovascular Drug Sectionfrom the 1st edition of Goodman & Gilman (1941)
Antiarrhythmic Drug Action • The pharmacological goal of antiarrhythmic drug therapy is to reduce ectopic pacemaker activity and modify critically impaired conduction • The ideal antiarrhythmic drug should be more effective on ectopic pacemaker and depolarized tissues than on normally depolarizing tissues • The ideal antiarrhythmic drug should decrease mortality • Unfortunately, many of the drugs presently available for treating arrhythmias may increase mortality
Antiarrhythmic Drug Action • All of the antiarrhythmic drugs act by altering ion fluxes within excitable tissues in the myocardium • The three ions of primary importance are Na+, Ca++, and K+ • The Singh-Vaughn Williams system classifies antiarrhythmic drugs agents by their ability to directly or indirectly block flux of one or more of these ions across the membranes of excitable cardiac muscle cells • The “Sicilian Gambit” classification includes the effects of drugs on other channels, receptors, and ion pumps
Luo-Rudy Model of the Cardiac Myocyte • Cardiac ventricular myocytes are actually composed of many different ion channels and pumps whose expression varies in different regions of the heart
Time course of myocyte ion fluxes(from G&G, Figure 34-3) Sodium channel blockers Calcium channel blockers Potassium channel blockers Cardiac glycosides
Electrical Activity in the Normal Heart (from Katzung) • The different action potentials in different regions of the heart reflect differential expression of ion channels, particularly Na+ channels • This leads to differential sensitivity to antiarrhythmic drugs
Arrhythmogenic Mechanisms • Enhanced automaticity • Can occur in cells with spontaneous pacemaker activity (diastolic depolarization) or cells that normally lack pacemaker activity (ventricular cells) • Afterdepolarizations and triggered automaticity • Normal depolarizations can trigger automaticity • Delayed afterdepolarizations (DADs) are associated with calcium overload • Early afterdepolarizations (EADs) are typically associated with potassium channel block and can lead to torsades de pointes • Reentry • The most common cause of arrhythmias • Can occur in any region of the heart where there is a region of non-conducting tissue and heterogeneous conduction around that region
Automaticity: Mechanisms for Slowing Pacemaker Rate(from Goodman & Gilman, 34-10) Drugs that Inhibit Automaticity b-Adrenergicblockers Na+ and Ca++ channel blockers Adenosine and muscarinic blockers K+ channel blockers
Afterdepolarizations and Triggered Automaticity(from Goodman & Gilman, 34-6) • DADs arise from the resting potential and result from calcium overload • EADs arise from phase 3 (repolarization phase) and result from prolonging action potential duration (typically from K+ channel block)
Reentry • The most common cause of arrhythmias • Can occur in any region of the heart where there is a region of non-conducting tissue and heterogeneous conduction around that region • Anatomically defined reentry refers to reentry that involves impulse propagation by more than one anatomical pathway between two points in the heart • Wolff-Parkinson-White syndrome • Atrial flutter • Paroxysmal supraventricular tachycardia • AV reentry and AV nodal reentry • Functionally defined reentry can occur in the absence of anatomically defined pathways • Atrial and ventricular fibrillation • Torsades de pointes
In the Common Mode of AV Nodal reentry, the anterograde impulse is slowed as it passes through the AV node The retrograde pathway of the reentrant circuit is fast. In the Uncommon Mode of AV Nodal reentry, the anterograde impulse is fast as it passes through the AV node The retrograde pathway of the reentrant circuit is slowed. Reentrant Mechanisms: AV Nodal Reentry
Animations of Reentrant Arrhythmias(can be found at NetPharmacology)
Classification of Antiarrhythmic Drugs • The Singh-Vaughan Williams (aka Vaughan Williams) classification system has been widely used to classify antiarrhythmic drugs based on mechanism of action and is still the primary system used for classification • The “Sicilian Gambit” is a newer classification system that takes into consideration the multiple antiarrhythmic actions that most drugs possess and the mechanism of a patient’s arrhythmia
Singh-Vaughan Williams Classification • Class I drugs, those that act by blocking the fast inward sodium channel, are subdivided into 3 subgroups based on their potency* (dissociation kinetics) towards blocking the sodium channel and effects on repolarization • Subclass IA High/intermediate potency as sodium channel blockers and prolong repolarization (prolong QT interval): Quinidine, procainamide, disopyramide • Subclass IB Lowest potency sodium channel blockers and may shorten repolarization (decrease QT interval): Lidocaine, mexiletine • Subclass IC The most potent sodium channel blocking agents (prolong QRS interval); have little effect on repolarization (no effect on QT interval): Flecainide, propafenone, moricizine *Potency is a reflection of kinetics of dissociation from the sodium channel; very high potency drugs dissociate slowly (recovery > 10 sec), whereas low potency drugs dissociate slowly (recovery < 1 sec)
Singh-Vaughan Williams Classification • Class II drugs act indirectly on electrophysiological parameters by blocking beta-adrenergic receptors (may slow sinus rhythm, prolong PR interval if adrenergic-dependent): Propranolol, esmolol, acebutolol • Class III drugs prolong repolarization (increase refractoriness, prolong QT interval, no effect on QRS interval, little effect on rate of depolarization): • Block fast outward K+ current: Amiodarone, sotalol, dofetilide • Block slow inward Na+ current: Ibutilide • Class IV drugs are relatively selective AV nodal L-type calcium-channel blockers (slow sinus rhythm, prolong PR interval): Verapamil, diltiazem • (*Note: Dihydropyridines have minimal effects on AV node depolarization)
Singh-Vaughan Williams Classification • Miscellaneous • In addition to the standard classes (IA, IB, IC, II, III, and IV) there is also a miscellaneous group of drugs that includes digoxin, adenosine, magnesium and other compounds whose actions do not fit the standard four classes
Advantages of the Vaughn Williams Antiarrhythmic Drug Classification System • It is a convenient means to classify the many antiarrhythmic drugs by their primary mechanism of action • It is a useful conversational shorthand • Drugs within a specific class or subclass often exhibit similar adverse effects • It is a useful starting point for deciding which drug to use for treating a particular patient
Class Toxicities of Antiarrhythmic Drugs (adapted from Woosley, 1991)
Relative Efficacies of Antiarrhythmic Drugs(adapted from Melmon and Morelli, 3rd ed.)
Drugs of Choice for Major Arrhythmias(Based on G&G 11th ed., Table 34-2) • Premature atrial, nodal or ventricular depolarization: • No drug therapy indicated • Atrial fibrillation, flutter, and PSVT: • AV nodal blockers to control ventricular response: • Adenosine, Class II, Class IV, digoxin • Note: AV nodal blockers may be harmful in WPW syndrome • Depending on arrhythmia: Class III, Class IA, Class 1C • Ventricular tachycardia (w/ remote MI): • Amiodarone, Class III, Class I • Ventricular fibrillation: • Lidocaine, amiodarone, Class III, Class I • Torsades de pointes: • Acute: Magnesium, isoproterenol • Chronic: Class II
Drawbacks of the Singh-Vaughn Williams Antiarrhythmic Drug Classification System • Drugs within a class do not necessarily have clinically similar effects • Almost all of the currently available drugs have multiple actions • The metabolites of many of the drugs may contribute significantly to the antiarrhythmic actions or side effects • Thus, an empirical approach is used by many clinicians to determine the most effective agent to use for a given patient
Sicilian Gambit Classification • An alternative classification system, known as the 'Sicilian Gambit', has been proposed that is based on arrhythmogenic mechanisms • This system identifies one or more 'vulnerable parameters' associated with a specific arrhythmogenic mechanism • A vulnerable parameter is an electrophysiological property or event whose modification by drug therapy will result in the termination or suppression of the arrhythmia with minimal undesirable effects on the heart • Unlike the Vaughan Williams classification system, this system can readily accommodate drugs with multiple actions • This multidimensional classification system is significantly more complex than the standard Vaughan Williams system, but provides a more flexible framework for classifying antiarrhythmic drugs based on pathophysiological considerations
Actions of Antiarrhythmic Drugs(adapted from Hurst’s the Heart, 10th ed.)
Lidocaine and mexiletine (Class IB) • Lidocaine is a widely used antiarrhythmic and local anesthetic. It is only used IV for treating arrhythmias because of first-pass metabolism. Mexiletine is lidocaine's orally active congener. • Both are used to treat acute, life-threatening ventricular arrhythmias. Although lidocaine has long been the first choice for treating ventricular arrhythmias, ECC/AHA 2000 guidelines for cardiopulmonary resuscitation recommend IV amiodarone before lidocaine for treatment of ventricular fibrillation or pulseless ventricular tachycardia. • Mexiletine does not prolong QT interval and can be used in patients with a history of torsades or DILQTs. Lidocaine is ineffective for prophylaxis of arrhythmias in post-MI patients. • Severe interactions can occur with co-administration of other antiarrhythmic agents, especially amiodarone. • The most frequent side effects are CNS including tinnitus and seizures, and occasionally hallucinations, drowsiness, and coma.
Procainamide (Class IA) • Effective against both supraventricular and ventricular arrhythmias (including atrial arrhythmias associated with WPW syndrome); can be administered IV and orally. • Its major metabolite, N-acetylprocainamide (NAPA), has predominantly Class III antiarrhythmic actions. Fast acetylators (~50% of the population) quickly convert procainamide to NAPA. • When procainamide is given orally, both procainamide and NAPA can contribute to the antiarrhythmic effects and toxicities; initial dosing should be conservative and monitoring of plasma concentrations is recommended. • Up to 40% of patients discontinue therapy within 6 months due to side effects. • Between 15 and 20% of patients develop a lupus-like syndrome, which usually begins as mild arthralgia, but can be fatal if allowed to progress. These symptoms are reversed if therapy is stopped, but patients need to be warned of the early warning symptoms so therapy can be aborted before serious problems develop.
Disopyramide (Class IA) • Useful for supraventricular arrhythmias, and ventricular arrhythmias only in patients with good ventricular function because of its negative inotropic effects. • The drug has anticholinergic effects which may be useful in some patients with vagally mediated paroxysmal supraventricular tachycardias, but the anticholinergic effects limit therapy in many patients.
Quinidine (Class IA) • Useful in treating supraventricular and ventricular arrhythmias, but there are significant risks of ventricular arrhythmias and other side effects. • Torsades is likely to be the major cause of quinidine syncope, which occurs in as many as 5-10% of patients within the first few days of therapy. Patients with a history of long QT, torsades, or hypokalemia should not be treated with quinidine. • Patients with heart failure can have proarrhythmias and digoxin interactions. • Common side effects include hypotension, GI problems (diarrhea and vomiting), and cinchonism (tinnitus, blurred vision, and headaches). • Quinidine is a potent inhibitor of hepatic CYP2D6 and is associated with more drug interactions than any other antiarrhythmic drug.
Propafenone (Class IC) • Used to treat symptomatic supraventricular arrhythmias and suppress life-threatening ventricular arrhythmias. • It is structurally similar to propranolol and has beta-blocking activity in addition to its sodium channel blocking activity. At therapeutic concentrations it can have significant beta-blocking activity which must be considered in patients with heart failure.
Flecainide (Class IC) • A potent fast inward sodium channel blocker used to treat symptomatic supraventricular arrhythmias and documented life-threatening ventricular arrhythmias. • Because of the risks of proarrhythmias identified in the CAST trials, the drug is not considered a first-line agent and should not be used in patients with impair ventricular function, myocardial ischemia, or recurrent myocardial infarctions. • The agent lowers ventricular function in most patients. It also raises the threshold of pacing and cardiac defibrillators and should be used with caution in patients with pacemakers or ICDs.
Verapamil and diltiazem (Class IV) • Useful in treating a variety of arrhythmias of atrial or supraventricular origin. They are also more effective than digoxin in controlling ventricular rate in patients with atrial fibrillation. • High doses can cause AV block or suppression of SA node, particular when used in combination with beta-blockers, digoxin or other drugs that inhibit the SA and AV nodes. Should be used with caution in combination with drugs that inhibit SA and AV function, lower LV function, or lower blood pressure. • Contraindicated in patients with heart failure, impaired LV function, sick sinus syndrome, heart block, severe hypotension or reentrant arrhythmias due to WPW or LGL syndrome. • Administration of these calcium channel blockers to patients with atrial tachycardias resulting from WPW can worsen the arrhythmia by facilitating antegrade conduction through the ancillary tract leading to ventricular fibrillation. • The most common side effect of verapamil is constipation. • Grapefruit juice is known to increase the plasma concentrations of verapamil because of its inhibitory effects on CYP3A4 in the gut wall.
Ibutilide (Class III) • Unlike other Class III agents, ibutilide prolongs repolarization by increasing inward sodium flux through the slow inward sodium channels. • It is used IV to rapidly convert atrial arrhythmias to normal sinus rhythm; it is the only agent indicated for this purpose. • Class IA or Class III drugs should not be used concurrently, or within 4 hours of ibutilide dosing, to avoid the possibility of DILQTS and torsades. • Ibutilide is contraindicated in patients with prolonged QT, torsades or other polymorphic ventricular arrhythmias, or who are taking drugs that prolong QT or are associated with torsades.
Sotalol (Class III and II) • The racemic d,l mixture of sotalol has both Class II and Class III effects. The l-isomer causes the beta-blocking effects, while the d-isomer causes the effects on prolonging the action potential. The l-isomer causes significant beta-blocking effects at doses well below those required for the antiarrhythmic effects of the d-isomer. • The combination of effects makes the drug effective in a variety of atrial and ventricular arrhythmias, though because of the proarrhythmic effects of Class III agents (torsades), high concentrations of the drug should only be used to treat life-threatening ventricular arrhythmias. • The drug is contraindicated in patients with QT prolongation, bradycardia, torsades, hypomagnesemia, hypokalemia, bronchospasm, pulmonary edema, heart failure, or AV block. • Because of the risk of arrhythmia or MI, abrupt cessation of drug therapy should be avoided; instead gradually reduce dosage over a 1 to 2 week period or substitute a different beta-blocker. • Drug combinations that enhance the pharmacological effects of sotalol (beta-blockade, QT prolongation, AV blockade) should be used with caution.
Amiodarone (Class III/other) • Though amiodarone is formally classified as a Class III antiarrhythmic, it has multiple actions and is more appropriately considered a "broad spectrum" antiarrhythmic. • Although it prolongs QT interval, its potential to cause proarrhythmias (torsades) is significantly lower than other Class III agents and it is one of the few antiarrhythmic agents to have consistently decreased mortality in many (but not all) clinical trials. • It is approved for use in refractory life-threatening ventricular arrhythmias, but its therapeutic role has been expanding to include a variety of arrhythmias ranging from supraventricular to ventricular. • Used IV, amiodarone is superior to lidocaine and other agents for the treatment of ventricular fibrillation (2000 ECC/AHA guidelines), and it is also used orally to suppress a variety of arrhythmias, even in combination with ICDs.
Amiodarone (cont.) • The safety of amiodarone for chronic therapy is controversial because of its variable and complex pharmacokinetics and many adverse effects, some of which can be fatal. • Without loading doses, it can take several weeks to months to achieve steady-state plasma levels. Similar, it can take many months to clear the drug, with an elimination half-life ranging from 26 to 107 days (mean of 53 days). • The most common serious adverse effects are pulmonary fibrosis and interstitial pneumonitis (2-15% of patients on chronic amiodarone), which is fatal in 10% of these patients. The pneumonitis is reversible if drug is stopped early on, thus clinical assessment and chest x-rays are required every 3 months.
Amiodarone (cont.) • Other adverse effects include: • GI disturbances, • hepatotoxicity (which can be fatal; 30% of patients have elevated serum liver enzymes), • hyperthyroidism and hypothyroidism (2-24% incidence; amiodarone is structurally similar to thyroid hormone and contains large quantities of iodine), • peripheral neuropathy (20-40% incidence, but reversible by lowering dose), • dermatological reactions (15-20%) including photosensitivity (10%), which can result in blue-gray skin color, and various visual disturbances (10%). • Virtually all patients on drug for more than 6 months develop corneal microdeposits which can eventually interfere with vision. • Amiodarone can interfere with the clearance of many drugs.
Digoxin (Misc.) • Digoxin is a cardiac glycoside that acts by inhibiting the sodium/potassium ATPase. This ion pump is ubiquitously expressed so digoxin affects a variety of excitable tissues including the heart, CNS and ANS. • Digoxin is used to control ventricular rate in patients with atrial tachycardias. • Digoxin increases vagal tone, thus inhibiting AV nodal conduction. • Dioxin can actually exacerbate atrial arrhythmias because it can cause calcium overload, but therapeutic efficacy is measured by the drug's ability to protect the ventricles by reducing the number of impulses passing through the AV node. • Digoxin has a relatively narrow therapeutic index and is known to interact pharmacokinetically with quinidine and other antiarrhythmic agents.
Adenosine (Misc.) • Adenosine is an endogenous compound that is an agonist for purinergic receptors. • It is given as a rapid IV bolus to acutely treat paroxysmal supraventricular tachycardia. • It potently blocks AV nodal conduction within 10-30 seconds of administration. • It has a half-life of elimination of 1.5-10 seconds. • Common side effects, which are short-lived, including facial flushing, dyspnea, and chest pressure.
Proarrhythmias • Proarrhythmias are drug-induced arrhythmias • Digitalis-induced proarrhythmias have been recognized for many years • Two recently recognized ventricular proarrhythmias seen with antiarrhythmic drugs: • Torsades de pointes (associated with drug-induced long QT syndrome (DILQTS)) • Quinidine (2-8% of patients, can occur at subtherapeutic doses) • Sotalol (common, but dose-dependent) • N-acetylprocainamide (metabolite of procainamide) • Amiodarone (DILQT is common, but torsades is uncommon) • Ibutilide (4-8%) • Dofetilide (1-3%) • CAST proarrhythmia • Flecainide (and encainide)
Torsades de Pointes ("twisting of the points") • Torsades is a polymorphic arrhythmia that can rapidly develop into ventricular fibrillation • Associated with drugs that have Class III and Class IA actions (potassium channel blockers and drugs that prolong repolarization) and cause Drug-Induced Long QT Syndrome (DILQTS) • Also seen with many other drugs (terfenadine, erythromycin, chlorpromazine under certain circumstances (see www.torsades.org for an up-to-date list) • FDA now requires in vitro HERG toxicity assays • Usually occurs within the first week of therapy • Preexisting prolonged QT intervals may be indicator of susceptibility • Potentiated by bradycardia (and can therefore be controlled by pacing) • Often associated with concurrent electrolyte disturbances (i.e. hypokalemia, hypomagnesemia)
ECG of Patient with Prolonged QT Interval and Torsades de Pointes (From Katzung)
CAST Proarrhythmia • Monomorphic, sustained ventricular tachycardia first recognized in CAST trials with encainide and flecainide • Patients with underlying sustained ventricular tachycardia, coronary artery disease, and poor left ventricular function (left ventricular ejection fraction <40%) are at greater risk to develop this form of proarrhythmia (these were the patients enrolled in the CAST trials)
Use(Rate)-Dependent Channel Blockade • Many of the sodium (Class I) and calcium (Class IV) channel blockers preferentially block sodium and calcium in depolarized tissues • Enhanced sodium or calcium channel blockade in rapidly depolarizing tissue has been termed "use-dependent blockade" • Responsible for increased efficacy in slowing and converting tachycardias with minimal effects on tissues depolarizing at normal (sinus) rates • Many of the drugs that prolong repolarization (Class III drugs, potassium channel blockers) exhibit negative or reverse rate-dependence • These drugs have little effect on prolonging repolarization in rapidly depolarizing tissue • These drugs can cause prolongation of repolarization in slowly depolarizing tissue or following a long compensatory pause, leading to repolarization disturbances and torsades de pointes
Affinity of Channel Blocker Drugs for Different Channel States (from Katzung) • Channel blocker drugs with higher affinity for the Active and Inactive states of the ion channel will demonstrate positive use-dependence • Drugs with fast dissociation kinetics (low potency) will only show efficacy in rapidly depolarizing tissue
Possible Mechanisms for Differential Affinity of Channel Blocking Drugs for Different Channel States (from Katzung) • Drug binding sites of use-dependent drugs might only be accessible to drug when the ion channel is in specific states • This might be due to the drug’s limited access to the drug-binding site from within the channel or because conformational ‘gates’ sterically block the drug’s access to the binding site