Download
1 / 1
20 likes | 172 Vues
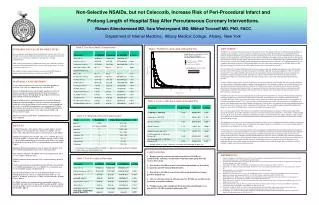
Non-Selective NSAIDs, but not Celecoxib, Increase Risk of Peri-Procedural Infarct and Prolong Length of Hospital Stay After Percutaneous Coronary Interventions. Rizwan Alimohammad MD, Sara Westergaard, MD, Mikhail Torosoff MD, PhD, FACC

E N D
Non-Selective NSAIDs, but not Celecoxib, Increase Risk of Peri-Procedural Infarct and Prolong Length of Hospital Stay After Percutaneous Coronary Interventions. Rizwan Alimohammad MD, Sara Westergaard, MD, Mikhail Torosoff MD, PhD, FACC Department of Internal Medicine, Albany Medical College, Albany, New York Table 1. Pre-Procedural Characteristics Figure. NSAID Use and Length of Hospital Stay DISCUSSION: INTRODUCTION & STUDY OBJECTIVES: NSAIDs use is associated with increased risk of cardiovascular events. This apparent risk may be mediated through inhibition of endothelial cyclooxygenase, which is required for production of prostacyclin I2 (PGI2). Reduction in endothelial PGI2 may promote vasospasm and platelet aggregation.(2) Another contributing factor may be non-selective NSAID-mediated reduction in cardioprotective anti-platelets effects of aspirin.(3) Non-selective NSAIDs (ns-NSAIDs) transiently block platelet cyclooxygenase and compete for binding sites with aspirin, reducing its’ effectiveness.(4) Upon ns-NSAIDs dissociation, platelet thromboxane A2 (TXA2) activity resumes with ensuing platelet aggregation and vasoconstriction.(4,9) Selective cox-2 inhibitor Celecoxib, by not competing with aspirin for platelet cyclooxygenase binding sites, has a theoretical advantage over ns-NSAIDs. Despite of this, high-dose prolonged Celecoxib use was also found to increase risk of cardiovascular events.(5,7) FDA and AHA/ACC recognize NSAID potential to increase cardiovascular risk. Warnings and guidelines were issued to make providers aware of this increased risk and discourage use of NSAIDs, especially in high risk population.(1) However, data on increased CV events with ns-NSAIDs and Celecoxib came from arthritis and gastro-intestinal trials, and was not obtained in populations of patients undergoing cardiac procedures.(6,7) We investigated effects of NSAIDs on outcomes in patients undergoing percutaneous coronary interventions. To our knowledge, ours is a first study addressing this important clinical question. We have analyzed a single tertiary center PCI experience. All consecutive patients were included. Adherence with the guidelines was high, with an overwhelming majority of patients treated with aspirin. Only minority of patients were on NSAIDs, mostly for musculoskeletal pain and arthritis indications. Patients on NSAIDs were younger, with reduced ejection fraction, and higher prevalence of prior myocardial infarction. This is in agreement with notion of increased risk of cardiac events in patients with rheumatologic conditions: these patients suffer more heart attacks, manifest lower ejection fraction, and may require cardiac interventions at a younger age. NSAIDs in our study were not associated with increased risk of post-PCI death. However, more post-PCI myocardial infarctions and longer hospital stay was noted in ns-NSAID, but not Celecoxib, treated patients. This association remained statistically significant when age, gender, ejection fraction, history of prior and post-procedural myocardial infarctions were adjusted for. In concordance with prior studies (7,10,11), we have observed longer hospital stay in older patients, and when co-morbidities were present, while female patients had reduced length of hospital stay. From the above it is apparent that our study population followed the trends observed by others (11) and met expected post-PCI outcomes. This concordance suggests biological plausibility and makes our observations on NSAIDs more convincing and unlikely occurring by chance. Why our study patients treated with selective cox-2 inhibitor Celecoxib had improved outcomes? Observational study cannot answer this question. One possible explanation is because a low dose of Celecoxib was used (219±83 mg daily). Another possible reason is the lack of Celecoxib attenuation of cardioprotective effects associated with low dose aspirin, which was used in almost all our patients. At the same time, anti-inflammatory and pain-reducing properties of Celecoxib might have allowed for an earlier patient discharge to home. The limitations of our study are its’ observational and retrospective character, lack of randomization, and low number of patients in ns-NSAIDs and Celecoxib groups. However, despite the low number of patients, vast differences in outcomes and high statistical significance of our findings are even more striking. To conclude, we have observed reduced incidence of post-angioplasty myocardial infarction and shorter hospital stay in patients receiving selective cyclooxygenase inhibitor Celecoxib, while patients treated with non-selective NSAIDs demonstrated opposite trends. Our findings suggest that until long-term placebo controlled randomized trials investigating cardiovascular events in NSAID-treated patients are completed, providers should abstain from using non-selective NSAIDs in this vulnerable population. Our data suggests that selective cyclooxygenase inhibitor Celecoxib, when used in low doses and for short period of time, may be associated with improved hospital outcomes in patients undergoing percutaneous coronary interventions. Regardless of the medication chosen, when cardiac patient with rheumatologic condition requires NSAID therapy, risks and benefits should be carefully weighed in and discussed with the patient. Non-steroidal anti-inflammatory drugs (NSAIDs) may increase risk of CV events through cyclooxygenase inhibition-mediated decrease in prostacyclin production and, in case of non-selective NSAIDs, by reducing ASA –afforded cardioprotection. FDA warnings and AHA/ACC guidelines discourage use of NSAIDs in patients with acute myocardial infarction, after coronary artery bypass surgery, or at risk of cardiovascular event. (1) We sought to evaluate hospital outcomes associated with NSAID therapy in patients undergoing percutaneous coronary interventions (PCI). MATERIALS AND METHODS: MATERIAL & METHODS: A single tertiary medical center experience from 2004 to 2006 was analyzed. The study was approved by the institutional IRB. Patients undergoing elective and emergent angioplasties with and without stenting were identified through NY State Percutaneous Interventions Registry. Demographic and procedural characteristics were defined according to the Registry. Data on NSAID use was collected through the institutional Pharmacy medication utilization database. Patients treated with rofecoxib and valdecoxib, drugs now withdrawn from the market, were excluded from the study. List of NSAID-treated patients was matched with NY State Percutaneous Interventions Registry. Charts of NSAID-treated patients were reviewed to identify doses of the administered NSAIDs and reasons for their usage. ANOVA, chi-square, Kaplan-Meier, and proportional hazard analyses were employed. Table 4. Factors Affecting Length of Hospital Stay Table 2. Utilization of Non-Steroidal Agents* RESULTS: Of 3043 PCI patients (29% females, 96% on aspirin, Table 1) only 69 (2%, Table 2) were treated with non-selective (ns) NSAIDs and 16 (0.5%) with Celecoxib. Twelve patients received more than one NSAID. NSAID-treated patients were younger (56+/-11 in ns-NSAID, 60+/-12 in Celecoxib, and 62+/-12 years old in “no NSAID” groups; p<0.001, Table 1). More NSAID-treated patients were females (p=0.0380), had a history of myocardial infarction (p<0.001) or reduced ejection fraction (p=0.003, Table 1). Majority of NSAID-treated patients were on aspirin 325 mg daily (78 of 79 ns-NSAID-treated patients and 15/15 in Celecoxib cohort). Most common indications for NSAIDs were musculoskeletal pain (35%) or “non- cardiac” chest pain (9%). NSAIDs treatment did not affect post-PCI in-hospital mortality (p=0.876, Table 3). However, post-procedural myocardial infarction (MI) was more common in ns-NSAID-treated patients (5% in ns-NSAID, 0% in Celecoxib, and 1% in “no NSAID” groups, p=0.002, Table 3). Post-procedural length of stay was also significantly longer in the ns-NSAID group (4.8±4.1 days), as compared to Celecoxib (1.3±0.5 days) or “no NSAID” groups (2.9±5.2 days; for live discharges, p<0.001, Figure, Table 3). Ns-NSAID treatment remained predictive of prolonged hospital stay (p=0.005) after adjustment for age (p=0.008), gender (p<0.001), ejection fraction (p<0.001), and history of previous (p<0.001) or post-procedural MI (p=0.001, Table 3). *) Hazard ratio of less than 1 indicates association with prolonged hospital stay *) One patient received three different NSAIDs; 12 patients received two different NSAIDS **) Aspirin dose was 325 mg daily or less CONCLUSIONS: REFERENCES: Despite growing awareness of deleterious effects of NSAIDs on cardiovascular outcomes, small number of patients undergoing PCI still receives these drugs. Non-selective NSAIDs, but not Celecoxib-treated patients are more likely to experience post-PCI myocardial infarction Non-selective NSAIDs, but not Celecoxib-treated patients incur longer post-PCI hospital stay. Adverse outcomes observed with non-selective NSAIDs are not affected by accounted co-morbid conditions. Pending results of the randomized trials, providers should limit use on non-selective NSAIDs in patients undergoing PCI. • 1. Bennet J, Daughtery A, Herrington D, et al, The Use of Nonsteroidal Anti-Inflammatory Drugs (NSAIDs). A Science Advisory From the American Heart Association. Circulation 2005 published online. • FitzGerald GA, Smith B, Pederson AK, Brash AR. Increased prostacyclin biosynthesis in patients with severe atherosclerosis and platelet activation. N Engl J Med 1984;310:1065-8 • 3. MacDonald TM, Wei L. Effect of Ibuprofen on cardioprotective effect of aspirin. Lancet 2003; 361:573-4 • Capone ML et al. Pharmacodynamic interaction of naproxen with low dose aspirin in healthy subjects. J Am Coll Cardiol 2005; 45:1295-301 • Bertagnolli MM et al. Celecoxib for the prevention of sporadic colorectal adenomas. • N Engl J Med 2006; 355: 873-84 • Bombardier C, Laine L, Reicin A, et al, for the VIGOR Study Group. Comparison of upper gastrointestinal toxicity of rofecoxib and naproxen in patients with rheumatoid arthritis. VIGOR Study Group. N Engl J Med. 2000; 343:1520-1528. • White WB, Faich G, Whelton A, et al. Comparison of thromboembolic events in patients treated with celecoxib, a cyclooxygenase-2 specific inhibitor, versus ibuprofen or diclofenac . Am J Cardiol. 2002;89:425-430. • White WB, Faich G, Borer JS, et al. Cardiovascular thrombotic events in arthritis trials of the cyclooxygenase-2 inhibitor celecoxib. Am J Cardiol. 2003; 92:411-418 • Konstantinopoulos PA, Lehmann DF. The cardiovascular toxicity of selective and non-selective cycloxyenase inhibitors: comparison, contrasts, and aspirin confounding, J Clin Pharmacol. 2005; 45:742-750. • Graham DJ, Campen D, Hui R, et al. Risk of acute myocardial infarction and sudden cardiac death in patients treated with cyclo-oxygenase 2 selective and non-selective non-steroidal anti-inflammatory drugs. Lancet 2005; 365: 475-481 • Faroukh ME, et al. Cardiovascular outcomes in high risk patients with osteoarthritis treated with ibuprofen, naproxen or lumiracoxib. Annals of the Rheumatric Disease. 2007;66:764-770. Table 3. Post-Procedural Outcomes