Download
1 / 68
690 likes | 1.05k Vues
Tackling the Public Health Challenge of Lassa fever. Dr S.A. Okogbenin Consultant Obstetrician, Irrua Specialist teaching Hospital. Lecturer, College of Medicine, Ambrose Alli University. Presentation outline. Introduction History Epidemiology Transmission Clinical course

E N D
Tackling the Public Health Challenge of Lassa fever Dr S.A. Okogbenin Consultant Obstetrician, Irrua Specialist teaching Hospital. Lecturer, College of Medicine, Ambrose Alli University.
Presentation outline. • Introduction • History • Epidemiology • Transmission • Clinical course • Pregnancy Issues • Response • Conclusion
Introduction • This is a viral haemorrhagic fever • caused by an arena virus • First discovered in Lassa town in Northern Nigeria • Also endemic in countries of the Manu river basin in West Africa. Sierra leone, Guinea and Liberia. • Zoonosis, with reservoir in the multimammate rat. Mastomys natalensis. • Naturally Causes disease only in humans.
History • Lassa mission hosp • In lassa town, • In the Yedseram river valley at the south end of Lake Chad. • Borno state, Northeastern Nigeria • 19th January 1969 • Laura Wine, 65 year old female • American missionary nurse • Described as very hardworking and hardly taking a holiday • became acutely ill, she had been in Lassa for four years • Had fever, back pain, sore throat
LAURA WINE. • Dr Hamer the only doctor at the station became worried over her deteriorating condition • She had • petechiae haemorrhage, • anuria. • Cloroquine, procaine penicillin • but no improvement • She started convulsing, • Flown to Evangel hospital formerly Bingham Memorial hospital in Jos.
Evangel hosp jos • Dr Jeanette Troup continued treatment • But Laura Wine • had internal haemorrhage, • went into shock • and DIED. • Charlotte Shaw, • nurse at the Evangel hospital in Jos • Described as kind loving and generous. • nursed Laura Wine intimately
Charlotte Shaw • On the day before Laurie Wine died, • Charlotte Shaw had given her oral toileting • cleaning her mouth with gauze wrapped round her index finger. • She had earlier that morning pricked her finger while plucking flowers for another patient. • Soon after Laura Wine died, Charlotte Shaw became ill. • Dr. Jeanette Troup, the female doctor again began to treat Charlotte Shaw. • Her note describes an illness similar to the one that killed Laura Wine. • 11 days after she became ill, Charlotte Shaw died.
Dr. Jeanette Troupe • Worried and confused by the death of Laura Wine and Charlotte Shaw, • decided to do an autopsy on Shaw. • She was assisted by the head nurse Penny Pinneo. • A week later Penny Pinneo became ill. • Realizing this illness does not respond to Chloroquine and Penicillin injections • Penny Pinneo was flown to New York. • Dr. Jeanette Troup herself later developed similar illness and died.
Penny Pinneo arrived New York alive. • Her specimens were sent to the Yale arbovirus research laboratory. • In Yale, a new virus was isolated by a team of Scientist led by jordi Casals after a couple of them got infected and one died. • Penny Pinneo survived and returned to Nigeria to continue her missionary work.
The virus that was isolated was named Lassa Virus. • This was the pattern for all haemorrhagic fevers. They were named after the town where the index case got infected. • In this case in Lassa town, in the Yeserdam river valley in the Southern part of lake Chad, Borno State, North Eastern Nigeria.
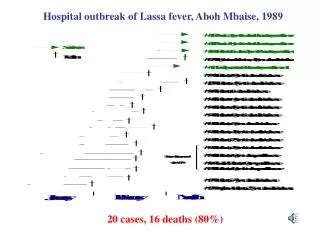
In this way, Lassa virus first announced itself, by claiming a team of missionary health workers. • That has continued to be the pattern of epidemic outburst. • Lassa Fever has been known to erase families teams of health workers and communities.
The Ihumudumu epidemic was equally dramatic. • In 1984 in Ihumudumu Community of Ekpoma, Edo state, • a woman had just died • while her burial arrangements were being made, her husband also died of a similar febrile illness.
They had 2 sons • One was a Medical doctor in Ekpoma • The second was a Chicago based Engineer. • They had all attended the burial. • They gave their parents befitting Burials • Afterall Esan men crave befitting Burials.
Shortly after, the medical doctor in Ekpoma became ill. • with fever, sore throat and proternuria, • a couple of days later he was bleeding from all orifices including injection sites • His Colleagues desperately tried to save him • A few days after burying his parents, he died.
With the death of a father, Mother, and a son, in a typical rural community in Nigeria. • Of course a young girl was implicated by the Community as the witch that was responsible after all she had “confessed”. • What happened to the Chicago based Engineer, he also attended the burial • Your guess is as good as mine.
The engineer who had travelled back to Chicago • became ill in America. • His blood was taken again to the Yale arbovirus laboratory. • He died on his hospital bed. • A few days later, the real witch was isolated. • It was the Lassa Virus.
In between these recorded epidemics, • it is believed that in many communities in Nigeria, Lassa fever continues to cause death undiagnosed and unchallenged. • It only comes to prominence if • it affects American missionary heath workers, • Chicago based engineers • other high ranking members of our country. • When it affects the voiceless, • it goes unannounced, • commonly taking refuge and misdiagnosed as resistant Malaria or Typhoid fever. • But for time constraints I would have told this audience about the Abakaliki, Jos, Plateau, Abuja and other epidemics in Nigeria.
Public health impact. • Wiping out of entire family members at once (Ihumudumun/Ekpoma). • High death rates among health workers (Lassa village, Jos, Imo, Abakalike) • Untimely death of friends, sympathizers and mourners as in the Abuja episode • Deafness: This occurs in 30% of survivors and results in impaired learning, frustration, and misery especially among students. • Panic in health Care institutions, among family members and community members
Public health impact. • Dissertations of Villages, and health care facilities • Reluctance to take up employment in health care institutions in endemic cares. • Loss of bread winner and Economic consequence on dependants • Stigmatization of affected Family: Courses on Family for evil done/witch craft accusation
Devastating effects of Lassa fever are beyond causing death, • it leaves in its wake misery, Panic, stigmatization, wrong accusation, Dissertation and economic deprivation.
The Upper level estimates of disease burden in Nigeria are suggested to be as follows: • At risk population of 51 million, • 3 million annual illness and • annual death of 58,330. (Richmond DJ, Baglole DJ. Lassa fever: epidemiology, clinical features, and social consequences. Br Med J 2003; 327:1271-5).
Because of the devastating effect • it has been categorized by the Centre of Disease Control as a category A select Agent for Bioterrorism • along with lethal agents like Bacilli Anthrax, Plague and Small pox. • This gives the virus an international appeal.
Since its isolation in 1969, • endemic in countries of the Manu river basin ie • Guinea, • Sierra Leone • Liberia. • There also reports in other countries • West Africa(Ghana) • Central Africa (Congo and Senegal). • It is also the most commonly exported viral haemorrhagic fever • Germany, America and the United Kingdom.
The dissemination of the infection can be assessed by prevalence of antibodies to the virus in populations: • Sierra Leone 8-52%, • Guinea 4-55% • Nigeria 21%. • In Nigeria the disease has now been reported in 24 states as at December, 2012.
In Serrie Leone, • 6-15% of cases of fever in hospital patients • 10-15% of hospital admissions are due to Lassa fever. • In Irrua Specialist Teaching Hospital about • 6% of patient with fever had PCR confirmed Lassa fever while • 6.8% of admissions to children’s emergency unit had suspected Lassa and 3.2% were PCR confirmed. • In University of Maiduguri Teaching Hospital, • 16% of patients with fever had serological evidence of previous, possibly recent infection.
Transmission • Lassa fever disease is a zoonosis • vector of transmission is the multimamate rat • known as mastomysnatalensis, • recognized by the multiple breasts on its ventral surface and • its relative hairless tail. • They are peridomestic in nature, • living around houses where they often feed and then return to surrounding bushes. • The breed copiously producing up to a dozen offspring in a single birth. • Once infected, the rats are infected for life and • transmit the virus to their offspring. • The rats are however not affected by the virus.
Transmission • There are 2 major modes of transmission, • Rodent to Human • inhalation of aerosolized virus, • ingestion of food or material contaminated by infected rodent excrement • catching and preparing the rats as food. • Human to human transmission • direct contact with blood, tissue secretion or excrement. • Needle stick or cuts facilitate the transmission. • Inhalation of aerosolized virus can also transmit the infection from human to human.
Clinical course • Once the virus enters human body, it is asymptomatic in 80% • It is only in 20% that it takes a complicated course of varied symptoms • incubation period of 1-3 weeks, • thereafter, illness last for another 3-weeks resulting in death or recovery.
Clinical features cont. • Symptoms -Because symptoms are varied and nonspecific, diagnosis is difficult. • Insidious onset - Fever, Malaise, headache, myalgia, back pain, • sore throat, cough, retrosternal pain, abdominal pain, vomiting, and diarrhea • conjunctivitis and sub conjuctival haemorrhage, facial and neck swelling. • hypotension • Bleeding occurs in less than 20% of those admitted.
Clinical features cont. • Renal failure • Neurological symptoms include tremors , convulsions and encephalitis • Permanent hearing loss occurs in one third of all cases • Breast and areola pain, tenderness, enlargement and tenseness. (in pregnancy alone)
Definition for a Suspected Case of Lassa • Fever > 38oC for LESS than 3 weeks AND • ABSENCE of a clinical response after 72 hours of anti-malarial treatment and/or a broad-spectrum antibiotic AND • 2 major signs OR • 1 major sign AND 2 minor signs
Surveillance for Viral Hemorrhagic Fevers in theMano River Union Countries 2 major signs or 1 major and 2 minor Minor Signs General malaise Headache Retrosternal pain Muscle or joint pain Vomiting Cough Sore throat Abdominal pain Diarrhoea Proteinuria Leucopenia < 4000/μL • Major Signs • Abnormal bleeding (from the mouth, nose, rectum, and/or vagina) • Edema of the neck and/or face • Conjunctival or sub-conjunctival haemorrhage • Jaundice • Spontaneous abortion • Buzzing in the ears or acute deafness • Persistent hypotension • Confirmed contact with a patient suffering from Lassa fever • Elevated liver transaminases (SGOT/AST)
Confirmatory test can be done only in 2 laboratories in Nigeria, • the Irrua Specialist Teaching Hospital • Lagos University Teaching Hospital virology laboratory of prof. Omilabu • private laboratory of Professor Agbonlahor in Benin City. • The Laboratory confirmation utilizes • Elisa test for antigen and 1gM antibodies • Reverse transcriptase PCR. • Viral Culture and Histochemistry are usually for research purposes.
Treatment. • The specific drug for treatment is Ribavirin which should be given intravenously within 6 days of symptoms. • Patients are best treated in isolated facilities. • Facilities for intensive care and renal dialysis • Personal protective equipment • Universal precautions.
Issues with pregnancy • 15% mortality in non-pregnant women • 30-60% in pregnant women • Perinatal mortality 90% • Abortion • Intrauterine fetal death • Late intrauterine fetal death
Issues with pregnancy. • The high maternal and perinatal mortality has been attributed to many factors. • Lassa virus has a high affinity for placenta and vascular tissues • Fetal immunity is low • maternal immunity diminishes in pregnancy. • The result is : • infected pregnant woman habours significantly higher viral load than in the non-pregnant population • high viral load correlates with poorer out come.
Lassa fever in pregnancy is an enigma. • With special challenges in diagnosis, management and consequences
Challenges of diagnosis Early LF Symptoms mimic Pregnancy Symptoms • Diagnosis and treatment is delayed with poorer outcome • Convulsions in late LF can mimic Eclampsia • Haemorrhage in LF can mimic Obstetric Haemorrhage. • Sepsis out look of LF can mimic Obstetric related sepsis • Viewed against the background that Eclampsia, Obstetric Haemorrhage and Sepsis are the 3 commonest causes of maternal mortality in Nigeria, • in settings of low index of suspicion • Where facilities are lacking for laboratory diagnosis, • many cases of LF may have been misdiagnosed • thus LF may be a cause, a HIDDEN cause of Maternal mortality.
LF accounts for 25% of maternal death in Serra leone. • In Irrua Specialist Teaching Hospital it accounts for 20% • This may be the picture in other Lassa fever endemic communities in Nigeria. • Yet maternal death due to Lassa fever ….not previously reported in Nigeria nor has its contribution to material mortality be acknowledged. • Lassa Fever could be a significant but hidden cause of maternal deaths in several communities in Nigeria.
Lassa Fever could be a significant but hidden cause of maternal deaths in several communities in Nigeria. • This is worrisome considering Nigeria has one of the highest maternal mortality rates which have seemingly defied intervention attempts.
Challenges in pregnancy. • 2 individuals involved, fetus and mother. • Fetus • Catastrophic, neonatal Lassa fever is rare. • IUD can be case defining. • High affinity for vascular tissues and placenta • Fetal immune system is still immature. • Perinatal mortality of 85-95%
Management • The issue is the presence of the fetus and placenta • Evacuation reported to improve outcome • Termination of pregnancy has been suggested • It improves response to ribavirin • Fetus is usually dead anyway • It improves overall maternal outcome. • These were mainly from sierrie Leone studies. Where termination was a main treatment modality.
Management cont • What if the fetus is alive. Is termination the most appropriate management? • Early sacrifice of the fetus was questioned • Optimum management in such instances need further evaluation • the big question here is what is optimum management of pregnant women infected with lassa fever.
To answer the question we reviewed 26s cases of PCR diagnosed lassa fever in pregnancy. • Our observations pointed towards new lessons that have implications for management and gives some direction and hope.
mortality • 26 RT-PCR confirmed cases. • 12 maternal deaths • 14 maternal survivors • 46.2% mortality • 6 of the 12 deaths occurred within 24 hours • 4 within 24-48 hours. • Ie 10/12 (85%) deaths occurred within 48hours. • Many of those with intrauterine fetal death could not achieve delivery before death.
Factors associated with mortality. • Intrauterine fetal death. • 7 women presented with IUFD, all died • 2 of the 7 women with spont. abortion died. • Viable pregnancy • 10 women came with viable pregnancy 9 survived • Of the 14 women who survived 9 came with viable pregnancy 5 had a spontaneous abortion
When patients presented with viable pregnancy, Treatment with ribavirin was significantly associated with survival • Patients with an intrauterine fetal death were significantly more likely to die irrespective of ribavirin use. • These preliminary findings suggested that presentation with a viable fetus may be predictive of improved maternal and fetal outcome and conservative management with ribavirin rather than evacuation should be considered. • Evacuation of the Uterus was fundamental to survival only when an intrauterine fetal death has occurred..”
This finding significantly changed the approach to management of pregnant women infected with Lassa virus. • Professor PardisSaberti • “If untreated, Lassa fever has extremely high fatality for pregnant women and nearly 100% fatality for their fetuses, as such, ribavirin is indicated even for pregnant women”. • American ribavirin registry which was designed to evaluate the potential human teratogenicity of prenatal exposure to ribavirin. • Findings after 5 Years of Enrollment, 2003- 2009 “Although the registry has not reached sample size goals, preliminary findings have not detected a signal indicating human teratogenicity for ribavirin
significance • IUFD….prognosis….rescue mission.. • Ribavirin, expedite delivery, bleeding problems • Fetus Alive ..prognosis…Evacuation may not be optimal. And need not be first option of management…..ribavirin and symptomatic • Even if baby becomes compromised • If fetus dies during treatment then commence process of evacuation. • After discharge…IUFD still possible(50%)…monitor fetus(ctg) deliver at 37 wks.
Summary of treatment • Co manage with physician, best isolated. • supportive care • Fluids • Monitor urine output • E/U/Cr, LFT, FBC,} correct as necessary. • Clotting profile. • Antibiotics, avoid gentamycin • Give Ribavirin • Conservative if the fetus is viable, • Expedite delivery if there is fetal demise • Breast symptoms improve as disease is being treated.