Download
1 / 59
610 likes | 940 Vues
The Future of Healthcare Delivery: An Introduction to Telemedicine. Erik Southard, RN, MSN, C-FNP Director of Special Projects Richard G. Lugar Center for Rural Health Terre Haute, Indiana. Introductions. Definition of Telehealth. Definition of Telemedicine. What is the internet?

E N D
The Future of Healthcare Delivery: An Introduction to Telemedicine Erik Southard, RN, MSN, C-FNP Director of Special Projects Richard G. Lugar Center for Rural Health Terre Haute, Indiana
Introductions. Definition of Telehealth. Definition of Telemedicine. What is the internet? Discussion of telemedicine applications. Statistics on telemedicine activity. Telemedicine programs throughout the state. Next steps. What’s going on now? Q & A. Presentation Objectives
Telemedicine and College • Can I be successful? • Many have gone before me (successfully). • Is this the right thing to do? • This can be expensive. • Fear of failure? • Is it sustainable? • Experimentation? • Encountering Naysayers. • Personal support, hard work, and collaboration? • Success.
Audience Participation • Who is currently involved with some form of telemedicine? • Who thinks that telemedicine is impractical and can’t be sustained? • If you have considered telemedicine, what is your greatest specialty need? • Can telemedicine help us improve access to care for Indiana and more specifically Indiana’s rural residents?
Lugar Center Mission • The mission of the LCTR is to prepare and train primary care physicians for successful rural practice and to expose individuals not yet decided on a career to the rewards of delivering health care services in a rural area.
Key Success Factors • Rural Training Track (RTT), a specially designed hands‑on curriculum for future rural health providers. • Commitment to a multidisciplinary team approach to providing health care. • Incorporation of computer and communications technology to support rural providers.
Importance of Technology • Professional isolation. • Lack of specialist support. • Continuing Medical Education.
How Technology Transforms Conventional Wisdom • Charles Duell, Commissioner, US Office of Patents, 1899. • “Everything that can be invented has been invented” • Thomas Watson, Chairman, IBM, 1943 • “I think there is a world market for maybe five computers.” • Ken Olson, Founder/Ceo, Digital Equipment Corp, 1977 • “There is no reason anyone would want a computer in their home.” • Bill Gates, Co-Founder, Microsoft, 1981 • “640 K ought to be enough for anybody”
Significant Advances of Technology Vacuum Tube (Lee De Forest, 1906) Transistor (ATT’s Bell Labs, 1947) Computers (1925) Satellite (1962) Fiber Optics (1966) Internet (1983, made available mid-1990’s) Digital Routing for voice and data (1990’s) Cell Phone High Speed
Telemedicine began .. . • In 1924, with the concept of a physician seeing his patient over the radio using a television screen. • First wave of telemedicine programs started in the 1950s with Wittson, Affleck, and Johnson. • Now in our third wave. • Most programs that began in the 1960s-1980s no longer exist.
Telemedicine Now • The 1990’s saw a doubling in number of two-way interactive video programs. • Teleradiology, store-and-forward, remains most common application. • Technology is rapidly changing and costs are decreasing. • Correctional is heaviest use. • Moving into private physicians use. • Expanding applications.
Telemedicine and Telehealth “Telemedicine and telehealth both describe the use of medical information exchanged from one site to another via electronic communications to improve patients’ health status” http://americantelemed.org/ICOT/Terminology.pdf
Types of Telemedicine • Synchronous-Describes interactive video connections because the transmission of information in both directions is occurring at exactly the same period. (Live Telemedicine) • Asynchronous-Describes store and forward transmission of medical images or information because the transmission typically occurs in one direction in time. (Store and forward telemedicine)
Store and Forward www.RuralConsult.com
No scheduling constraints. Less burdensome technical requirements. Low connection and equipment costs. (POTS) Information stored centrally, more secure. Limited Specialties. Delay in getting feedback. No patient provider interaction. Incomplete view of the case. Store and Forward ADVANTAGES DISADVANTAGES
Live Telemedicine Equipment • General Examination Camera • E-Stethoscope • ENT Scope • Ophthalmoscope • X-Ray Digitizer • 12 lead ECG machine • Spirometer
Multiple specialty use. Interactive. High quality video and audio. Patient provider relationship. Scheduling constraints. High equipment costs. Expensive line charges. Live Telemedicine ADVANTAGES DISADVANTAGES
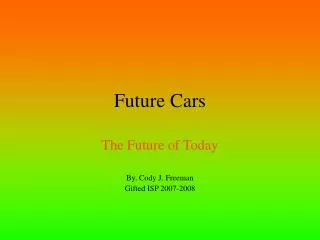
Telemedicine Equipment Power ZoomPush-button 1-50x zoom allows both close focus and wide angle images. Auto FocusThe camera automatically stays in focus for ease of use. Freeze FrameFreeze frame produces the clearest possible image, making it ideal for both low- and high-bandwidth solutions. Accurate ColorsOne button white balance sets highly accurate colors quickly and easily. PolarizationElimination of surface skin reflection allows camera to see into epidermal layers. Touch and ViewThe AMD-2500 includes manual or automatic iris control to maximize image brightness. AMD 2500 General Examination Camera
Quality Images Pictures taken by AMD 2500 General Examination Camera
Type of Telehealth Activities Reported from HRSA Telehealth Inventory
Why Telemedicine? • Access • Provide primary healthcare that would not be available otherwise. • Specialty care consultations for isolated specialists, practitioners, and other health care professionals. • Eliminate expensive travel and isolation. • Reduce need to move patient. • CME for isolated health care providers.
Telemedicine Settings • Rural • Schools • Clinics • Hospitals • Prisons • Nursing Homes/Assisted living
Emerging Applications • Telepharmacy • Broader Home Health • Remote Surgery
Core Principles of Telemedicine • Its only a tool. • Must have a program champion. • Must be integrated into established clinical operations and routines. • Physician-patient relationships must be preserved.
Creating a Successful Program • Define the need. • Who are the key people that need to participate. • What services are needed. • What are the most logical sites or personnel to have involved? • When are the services needed? • How are the services best supported?
Assess Equipment Options • Store and Forward. • Live Telemedicine. • Necessary Peripherals.
Assess Transmission Options • Plain Old Telephone System (POTS) • Integrated Services Digital Network (ISDN) • Internet Protocol (IP) • Digital Subscriber Lines (DSL) • OCRA • OUCC
Estimate Costs • Employees. • Line Charges. • Equipment Costs. • Reimbursement and Revenue Streams???
Address Policy Issues • Health Insurance Portability and Accountability Act (HIPAA) • Joint Commission on the Accreditation of Healthcare Organizations (JCAHO) • Licensure • Liability
Operational Organization • Institutional Commitment. • Staffing Concerns. • Map out clinical, technical, and administrative activities.
Implementation Timelines • Create Protocols. • Legal Counsel review. • Solicit equipment bids. • Research equipment. • Order equipment and telecom. lines. • Preliminary testing. • Training site coordinators and staff.
Outcome Measures • Clinical Outcomes. • Process Measures. • Participant Acceptability. • Costs.
Telemedicine in Indiana • Programs are few in number. • Acceptance among providers is growing. • Indiana, a leader in electronic medical records, is working to increase telemedicine activity. • Six main programs.
NeuroPsychOnline • Started in 2003. • Completed 250 consults. • Provides online interactive cognitive rehabilitation services for those with brain injury from injury, disease or other neurological anomaly. • For more information contact Odie Bracy at (317) 257-9672.
Community Behavioral Care Services • Psychiatric Consults. • Connects North Campus to South Campus. • Assessments for admission. • Small program but looking to expand. • For more information contact Travis Lozier, IT Site Director (317) 621-7987
St. Vincent Health • Home monitoring project for congestive heart failure patients & palliative care. • Distance learning and education programs. • https://secure.stvincent.org/distancelearning/default.aspx • Live interactive telepsychiatry services. • For more information contact John Winenger (317)415-6159.
St. Vincent Health • Remote Monitoring for Group Homes starting in March 2007. • Tele-OB services with CAH (In progress). • EMS intermediate class with St. V. Williamsport via remote connection. • NP to MD consults via video connection to Clay City.
Clarian Telemedicine • Program began in 2003 with HRSA grant. • Offers live, interactive consults between patients and providers. • Clarian Telemedicine has facilitated over 756 cases and completed 249 live interactive consults. • Clinic sites in Bedford, Terre Haute, South Bend, Fort Wayne and Evansville. • For more information contact Rebecca Salley at (317) 278-0195.
RuralConsult.com • Store and forward telemedicine program. • Created by Union Hospital’s Richard G. Lugar Center for Rural Health in December of 1999. • System provides online access to 12 medical specialists as well as continuing medical education credits. • RuralConsult.com has over 150 registered providers and has completed over 350 consults. • For more information contact Hicham Rahmouni, IT Specialist at (812) 238-7479.
Telehealth Advisory Consortium • Formed by Greg Beck in May 2005. • Volunteer group of more than 20 members representing 10 different organizations. Mission: To advance telehealth services in Indiana communities through collaboration, advocacy and education. www.indianatac.org
Fostering Collaboration Indiana Rural Health Association Annual Conference June 6th and 7th will feature a telemedicine track sponsored by ISDH and the Telehealth Advisory Consortium.