Download
1 / 38
380 likes | 394 Vues
Learn pathophysiology, manifestations, lab tests, diagnosis, care priorities, and nutrition therapy for liver, pancreas, and gallbladder diseases. Understand hepatitis causes, prevention, and assessment of cirrhosis.

E N D
Nursing Care and Interventions with Diseases of the Liver, Gallbladder & Pancreas Keith Rischer RN, MA, CEN
Today’s Objectives… • Review pathophysiology and systemic manifestations of the inflammatory response. • Compare and contrast pathophysiology & manifestations of diseases of the liver, pancreas and gallbladder. • Interpret abnormal laboratory test indicators of liver, pancreatic and gallbladder function. • Identify the diagnostic tests, nursing priorities, and client education with diseases of the liver, pancreas and gallbladder. • Analyze assessment data from clients with cirrhosis to determine nursing diagnoses and formulate a plan of care for clients with diseases of the liver, pancreas and gallbladder. • Prioritize assessment based nursing care for clients experiencing chronic pancreatic or gall bladder disease. • Integrate nutrition therapy in care of clients with hepatic, pancreatic or gallbladder disease.
Inflammatory Response • Occurs in response to injury • Localized • Immediate • Beneficial • Appropriate level of response • Non Specific
What is a Mast Cell? • Bag of Granules • Located in connective tissue • close to blood vessels • Histamine released • Increase blood flow • Increase vascular permeability • Binds to H1, H2 receptors
Causes • Bacteria-viral • Trauma • Lacerations • Allergic response • Bites • Burns
Purpose of inflammation • Neutralizes and Dilutes Toxins • Removes necrotic materials • Provides an environment for healing
Systemic Manifestations of Acute Inflammation • Fever/chills • Benefits • Increased killing of microorganisms • Increased phagocytosis by neutrophils • Increased activity of interferon • Leukocytosis • Plasma Proteins
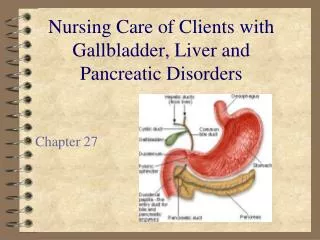
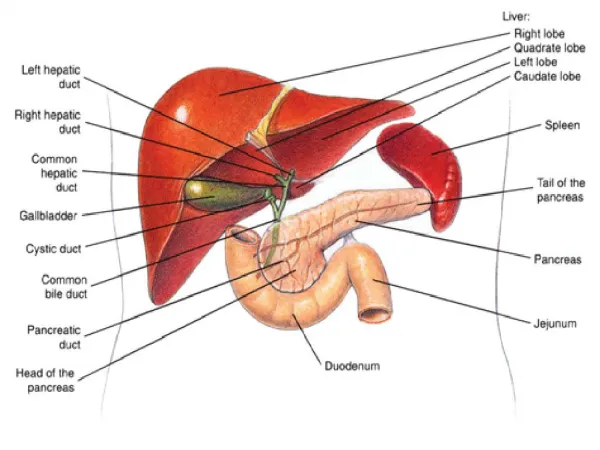
Liver Produces bile…elimination of bilirubin Drug/hormone metabolism CHO-fat-protein metabolism Clotting factor synthesis Storage of vitamins & minerals Gallbladder Store & concentrate bile Pancreas Endocrine Exocrine Patho Review
Hepatitis Definition: • Inflammation of the Liver Causes: • Viral (most common) • A, B, C, D, E • Toxic • Amiodorone, Tylenol, statins • Alcohol
Hepatitis A THINK FECAL-ORAL Etiology: Hepatitis A Virus • Incubation period: 15-50 days • Duration: 60 days • Young children asymptomatic • No chronic carrier…virus in feces during incubation pd. Before sx apparent Transmission: Fecal-Oral • Outbreaks occur by contaminated food/drinking water • Male homosexuals • Poor hygiene, improper handling of food, poor sanitary conditions • HAV found in feces 2 or more weeks before onset of sx and up to one week after onset of jaundice
Hepatitis A: Prevention • Good hygiene • Water treatment • Hepatitis A vaccine • booster 6-12 mos after first dose • Immunoglobulin before exposure or within 2 weeks after exposure • protects about 2 months
Hepatitis B THINK BODY SECRETIONS-BLOOD Etiology: Hepatitis B Virus • Incubation period: 48-180 days (mean 56-96) • Chronic & carrier status Transmission • Exposure to infected blood, blood products or body fluids • Found in most body secretions • Perinatal: mother to baby (10-85% liklihood) • 90% become chronic carrier…25% mortality as adults • Percutaneously (IV drug use, needle sticks) • Nurses at risk! • STD-30% cases r/t heterosexual activity • Major source of spread are healthy, chronic carriers
Hepatitis B: Prevention Hepatitis B vaccine • series of 3; use of HBIG for post-exposure prophylaxis • Screening of donor blood • Use of disposable equipment • Sterilization of non-disposable equipment • Abstinence/condom use • Needle exchange programs • Use of standard precautions and PPE
Hepatitis C THINK BLOOD-IV DRUG USE Etiology: Hepatitis C Virus • Incubation period: 14-180 days (mean 56) • Sx persist 2-12 weeks • Most common cause of chronic hepatitis, cirrhosis, liver CA • Most are asymptomatic carriers-spread to others Transmission • Percutaneous-contaminated needles • Bloodborne pathogen • Before 1990 most cases due to contaminated blood • IV drug use, needle sticks (tattoo/body piercing) • Perinatal/sexual contact uncertain
Hepatitis C:Prevention • Screening of donor blood • Use of disposable equipment • Sterilization of non-disposable equipment • Abstinence/condom use • No vaccine or use of IG at this time
Chronic Hepatitis Responsible for most cases of cirrhosis, liver CA • HCV responsible for 80% cases • Smolders over years…silently destroying liver cells Most asymptomatic but then develop… • Malaise • Easy fatigability • Jaundice • Hepatomegaly
Hepatitis-Cirrhosis: Laboratory Assessment • AST-Aspartate aminotransferase • ALT-Alanine aminotransferase • ALP-Alkaline Phosphatase • Total bilirubin • Albumin • Ammonia • INR-Prothrombin time (PT)
Hepatitis-Cirrhosis: Early Clinical Manifestations • Fatigue • Significant change in weight • Gastrointestinal symptoms • Abdominal pain and liver tenderness • Pruritus
Hepatitis-Cirrhosis: Late Clinical Manifestations • Jaundice and icterus • Dry skin • Rashes • Petechiae, or ecchymoses (lesions) • Peripheral dependent edema of the extremities and sacrum
Mortality 1% Higher w/elderly & other underlying debilitating disease Hepatic failure Ascites Chronic hepatitis Cirrhosis Hepatic cancer Liver transplant Hepatitis: Endstage Complications
Hepatitis: Care Planning Priorities • Fatigue • Physical rest • Nutritional intake • Sm. Frequent meals • High carb-low fat • Nausea • Knowledge deficit • Avoid Tylenol, ETOH • Diet • Drug therapy • Interferon: SQ and po
Patho Inflammation Causes ETOH Hepatitis C Cirrhosis
Massive ascites Hepatomegaly (liver enlargement) Assess nasogastric drainage, vomitus, and stool for presence of blood Bruising, petechiae, enlarged spleen Neurologic changes Cirrhosis: Physical Assessment
Complications: Cirrhosis • Portal hypertension • Ascites • Bleeding esophageal varices • Coagulation defects • Vitamin K not absorbed • Jaundice • Primary liver disease • Intra-hepatic obstruction • Portal-systemic encephalopathy with hepatic coma • Ammonia levels • lactulose
Cirrhosis: Care Planning Priorities • Excess fluid volume • Diuretics • Low sodium diet • Paracentesis • Risk for imbalanced nutrition • Chronic pain • Risk for impaired skin integrity • Potential for hemorrhage
Cirrhosis: Nursing Priorities • Fluid-electrolyte management • Na+, K+, BUN, • I&O • Bleeding precautions • Assess INR-PT-platelet-Hgb • Monitor ortho’s • Assess sx bleeding • Neurologic assessment/monitoring • Assess ammonia levels • Monitor LOC/orientation • Fall risk
Liver Case Study • 67yr male • PMH: DMII, ETOH abuse, high cholesterol, PAF, CRI, Kidney CA 2001, cardiomyopathy • CC: painless jaundice that started appx 4 weeks ago when wife noted eyes becoming yellow…did not seek medical care right away • Became visibly jaundiced, developed dark urine, stools light in color, weak but no N-V-D or abd pain • MD office: Bili of 25. Amiodorone and Lipitor DC’d. US abd done • Hepatic duct dilation w/further testing found to have pancreatic mass
Incidence/Prevalence 20% US population impacted Risk Factors Sedentary lifestyle Obesity Middle aged Caucasian women High cholesterol Estrogen-BCP Patho Inflammation Gallstones Cholesterol/bile salts Cystic duct obstruction or may lie dormant in GB Acute Cholecystitis-Cholelithiasis
Upper abd. pain RUQ or epigastric Rebound tenderness Episodic or vague Radiation to right shoulder Triggered by high fat/large meal Anorexia N&V Fever Acute Cholecystitis-Cholelithiasis:Clinical Manifestations (chart 63-1 p.1398)
Acute Cholecystitis-Cholelithiasis Diagnostic & Interventions • Laboratory Findings • WBC • Diagnosis • CT or US • Interventions • Nonsurgical • Diet • Pharmocological • Surgical • laparoscopic
Acute Cholecystitis-Cholelithiasis: Nursing Priorities • Acute pain • Impaired skin integrity • Risk of infection • Knowledge deficit • Pain management • Diet therapy • Low-fat • Smaller, more frequent meals • Wound/incision care • Signs of infection • Activity restrictions • Follow-up care
Pancreas Functions as both exocrine/endocrine gland Patho Lipolysis Proteolysis Necrosis of blood vessels Inflammation Theories of enzyme activation ETOH Acute Pancreatitis
Biliary obstruction Cholecystectomy-postop Trauma Familial/genetic Incidence/Prevalence ETOH-holidays Women-after cholelithiasis Mortality 10% Higher w/elderly & postop Pancreatitis: Etiology
Abdominal pain-LUQ/epigastric Radiation to back, left flank/shoulder Nursing Assessment Abdomen Respiratory Neuro VS Pancreatitis:Physical Assessment
Pancreatitis:Laboratory/Diagnostic Assessment • Lab • Amylase • Lipase • Glucose • Bilirubin • WBC • Radiographic • CT • MRI
Complications of Acute Pancreatitis p.1404 Table 63-2 • Pancreatic infection • Hemorrhage • Hypovolemic or septic shock • Respiratory • Pleural effusion • Pneumonia • Acute Resp. Distress Syndrome (ARDS) • Multisystem organ failure • Disseminated intravascular coagulation • Diabetes mellitus
Pancreatitis: Nursing Priorities • Acute Pain • PCA • Imbalanced nutrition • Nothing by mouth in early stages-7-10 days • Antiemetics for nausea and vomiting • Total parenteral nutrition • Small, frequent, moderate to high-carbohydrate, high-protein, low-fat meals • Knowledge deficit • ETOH avoidance • Recurrent abd pain • Jaundice-clay colored stools-darkened urine
Pancreatic Carcinoma • Etiology • Smoking • Elderly 60-80 years • Genetic • Patho • Primary vs. metastatic • Aggressive mets