Download
1 / 54
560 likes | 855 Vues
Laparoscopy- anaesthetic concerns . Dr. S. Parthasarathy MD., DA., DNB, MD ( Acu ), Dip. Diab . DCA, Dip. Software statistics PhD ( physio ) Mahatma Gandhi medical college and research institute , puducherry – India . What is it ?? .

E N D
Laparoscopy- anaesthetic concerns Dr. S. Parthasarathy MD., DA., DNB, MD (Acu), Dip. Diab. DCA, Dip. Software statistics PhD (physio) Mahatma Gandhi medical college and research institute , puducherry – India
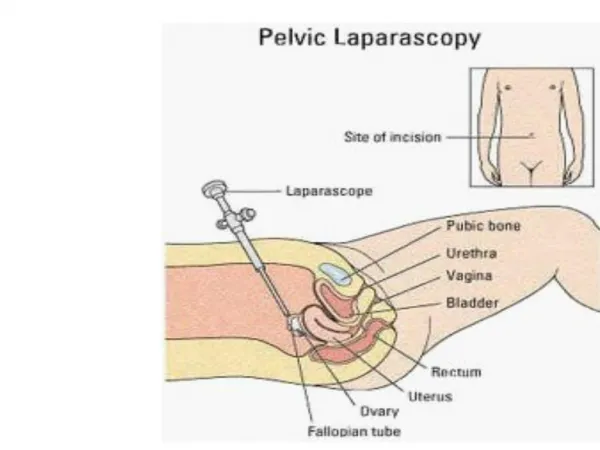
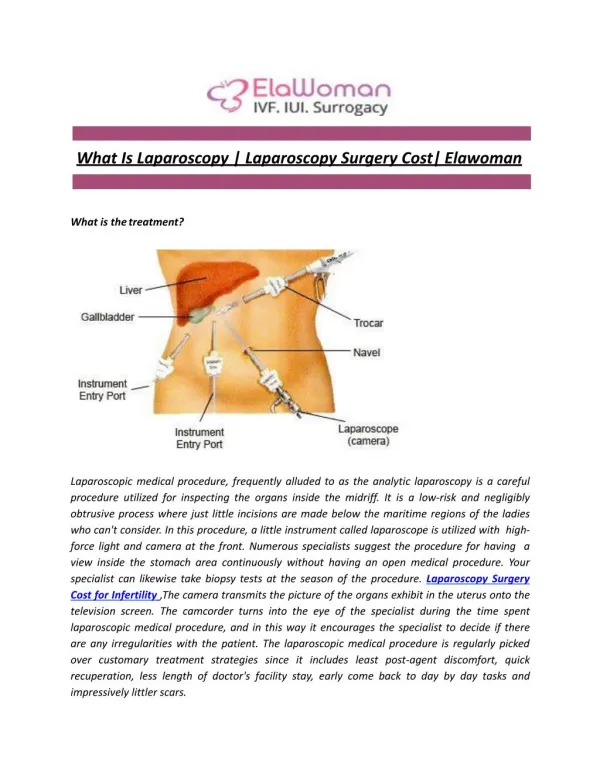
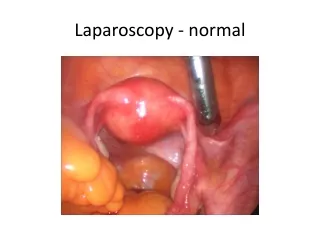
What is it ?? • Laparoscopy (or peritoneoscopy) is a “minimally invasive” procedure allowing endoscopic access to the peritoneal cavity after insufflation of a gas (CO2) to create space between the anterior abdominal wall and the viscera. • Laparoscopic surgery can also be extraperitoneal. It can also be gasless with abdominal wall retraction, • Hand assisted
Some history • Laparoscopy introduced in 20 th Century • 1975 : first laparoscopic salpingectomy • 1970 -- 80 : used for gyne procedures • 1981: Semm, from Germany,1st lap appendectomy • 1989: laparoscopic cholecystectomy
major benefits • Small incision • reduced postoperative discomfort, • shortened recovery rates, • lower incidence of post operative wound infections • Less post op pulmonary complications • shorter in-patient stay
Advantages • Obesity and bariatric surgery • Pulmonary diseases
Disadvantages • Higher equipment costs • May be longer time of surgery • Cannot do • Positioning and Pneumoperitoneum cardiopulmonary effects
Contraindications • Diaphragmatic hernia • Acute or recent MI • Severe obstructive lung disease • Increased ICP • V – P shunt • Hypovolemia • CCF • Valvular heart diseases • CHAVI
Three specific problems • Positioning • Pneumoperitoneum • CO2 insufflation
Positioning • Trendelenberg and reverse Trendelenberg and its effects • ‘well leg compartment syndrome’ induced by the combination of • impaired arterial perfusion to raised lower limbs, • compression of venous vessels by lower limbs supports, • reduced femoral venous drainage due to pneumo peritoneum.
Risk factors • Risk factors include surgery > 4 h duration, muscular lower limbs, obesity, peripheral vascular disease, hypotension, and steep Trendelenburg positioning Get up after two hours and go back again
pneumoperitoneum • CO2 insufflation --- intra-abdominal pressure (IAP) climbs. • Normal IAP = 0 – 5 mmHg • Upto 10 – ok • More than 15 – problems start • Individual systems affected
Cardiovascular effects • systemic vascular resistance (SVR) is increased 1.Mechanical compression of the abdominal aorta 2.Production of neurohumoral factors such as vasopressin 3.activation of the renin–angiotensin–aldosterone axis. IVC compressed Positioning can exacerbate
Steps to decrease CVS effects • Healthy patients appear to tolerate these hemodynamic effects well • What will decrease?? • the lowest insufflation pressure • vasodilating agents, centrally acting alpha-2 agonists. • appropriate intravenous fluid loading
RS • The upward pressure elevates the diaphragm, compresses the lungs, and impedes expansion of the lungs and chest cavity • decreased functional residual capacity – atelectasis – V/Q mismatch • Thoracopulmonary compliance may be decreased by up to 50% during pneumo peritoneum. • Exacerbated by positioning • The changes with anesthesia and laparoscopy can be partly offset by applying PEEP – but hemodynamics ??
Why should carbon dioxide ?? • Noninflammable • Rapidly excreted via the lungs • CO2 embolization is less (200 ml Vs 20 ml for air ) • medical grade CO2 is readily available • inexpensive. • CO2 levels can be measured
But CO2 is not inert • It gets convertedto carbonic acid in moist peritoneum – local pain • it can remain in gaseous form intra peritoneal after laparoscopy, causing referred shoulder pain. • Blood - Hypercarbia -- hypertension, tachycardia, cerebral vasodilation, and respiratory acidosis. Insufflations flow rate should be low, initially 1-1.5 Ltr/min of CO2
Splanchnic effects • Blood flow to the kidney and liver is significantly compromised with increasing IAP • 20 mm Hg ---- 25 % GFR decrease
Neurological effects • An elevated IAP causes an increase in intra-cerebral pressure (ICP) by limiting cerebral venous drainage as a consequence of raised intra-thoracic pressure CPP ?? On cardiac output POCD !!
Preanaesthetic preparation • Consent and readiness for laparotomy • The cardiac and pulmonary status of all patients should be carefully assessed • Premedication is usually not necessary except in anxious patients. • Atropine can be used for premedication to prevent vagally mediated brady arrhythmias • PONV prophylaxis • PONV
Monitoring • Pulse rate • Continuous ECG • Intermittent NIBP • Pulse oximetry (SpO2) • Capnography (EtCO2) • Temperature • Intra abdominal pressure • Pulmonary airway pressure • Others --- be vigilant like
Controlled GA with ETT – WHY ?? • Less gastric acid aspiration, • allows optimal control of CO2 • facilitates surgical access ---------------------------------------- • No mask ventilation • Ryles tube – gastric distension for view, prevention of gastric injuries
zone 4 opened , zone 3 increased, zone 2 becomes three in increased IAP. • The application of PEEP prior to Pneumo peritoneum is supposed to stop the lung changes • All so called changes due to PEEP will be acceptable if we have adequate intravascular status
laryngeal mask airway (LMA) • controversial due to the increased risk of aspiration • difficulties encountered when trying to maintain effective gas transfer while delivering the higher airway pressures • Still a lot of RCT s prove the use of proseal LMAs in lap surgeries
nitrous oxide • The use of nitrous oxide- controversial • produce bowel distension during surgery • increase in PONV • Halothane increases the incidence of arrhythmia during laparoscopic surgery, especially in the presence of hypercarbia
Remifentanyl – PCV • Extremely painful - insufflation • But surgery is short hence remifentanyl is ideal. • Pressure controlled modalities affords higher instantaneous flow peaks, • minimizing peak pressures, • improved alveolar recruitment and oxygenation in laparoscopic surgery for obese patients
Combined spinal epidural anesthesia forlaparoscopic appendectomy in adults: A case series • management of pneumo peritoneum, • achieving adequate level of analgesia • Problem of shoulder tip pain, • provision of postoperative pain relief • prevent deterioration of respiratory mechanics, • ambulation as early as possible. • Possible with GA ??
Spinal • Spinal anaesthesia with Hyperbaric Bupivacaine and Fentanyl is adequate and safe for elective laparoscopic appendectomy in healthy patients but careful evaluation of the method is needed particularly in cardio respiratory conditions. • Saudi Journal of Anaesthesia Vol. 6, Issue 1, January-March 2012
M Ravishankar et al • In a conscious patient undergoing laparoscopy with pneumoperitoneum, under spinal anaesthesia, the preserved inspiratory diaphragmatic activity maintains ventilation and, the gas exchange within physiological limits. Hence it is a safe alternative to general anaesthesia. Who said this ?? • J AnaesthesiolClinPharmacol. 2010 Oct-Dec; 26(4): 475–479. • Respiratory Changes During Spinal Anaesthesia for Gynaecological Laparoscopic Surgery
Previous slide and concepts 1Mechanical compression of the abdominal aorta 2.Production of neurohumoral factors such as vasopressin 3.activation of the renin–angiotensin–aldosterone axis. Using epidural and cutting off all symp. Afferents will correct all the above instead of using separate hypotensives
Ephedrine ok • Phenylephrine ??
Complications • CO2 emphysema • Capnothorax • CO2 embolism • Trochar may cause abdominal vessel injury, GIT perforation, hepatic and splenic tear and omental injury. • Extraperitonealinsufflation of CO2 • Pneumothorax pneumomediastinum and pneumopericardium • IPEEP
Treatment • Most of these cases – • 100 % oxygen., • Cut off nitrous • IVF and supportive measures
Endobronchial intubation • Cephalad displacement of the diaphragm during pneumoperitoneum result in cephalad movement of carina leading to endobronchial intubation
GAS EMBOLISM • Direct insufflation of gas into a vessel by misplaced trochar or veress needle. • Small bubble of gas carried through injured vein at operative site • Large gas absorption into portal circulation may be caused by very fast rate of gas flow and very high intra abdominal pressure
CARDIAC ARYHTHMIAS • Patient undergoing laparoscopy are prone to develop cardiac arrythmias due to high PCO2 and raised vagal tone . • Other complications • Darkness in the OR • Regurgitation • DARE – IPEEP
Insufflator Gas used N2O /CO2 /Argon /He/ Air Preferred gas : CO2 Working pressure : 12 to 14 mm Hg Slow inflation of 1 liter / minute (Air & O2 –risk of embolism high. N2O –bowel distension,risk of explosion,PONV. He & Argon not available here- embolism)
Post op management • O2 administration for couple of hours to prevent alveolar hypoxia as CO2 excretion continues • Energetic care for prevention of sickness must be taken as PONV can jeopardize all the benefits of laparoscopy and anesthesiologist gets total blame . • Proper warming of patient. • Attention must be paid for pain relief.